Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Smoke-Free Evironments ChileDocumento8 páginasSmoke-Free Evironments ChileKhairunnikmah ShaumiAinda não há avaliações
- Agra RokokDocumento18 páginasAgra RokokAlif HastrianandaAinda não há avaliações
- Ottawa Ankle Rules WikipediaDocumento3 páginasOttawa Ankle Rules WikipediaKhairunnikmah ShaumiAinda não há avaliações
- Ottawa Ankle Rules WikipediaDocumento3 páginasOttawa Ankle Rules WikipediaKhairunnikmah ShaumiAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- HypocalcemiaDocumento2 páginasHypocalcemiaRachel Frances SorillaAinda não há avaliações
- Physiotherapy in Leprosy: Presented byDocumento20 páginasPhysiotherapy in Leprosy: Presented byvyomphysio201050% (2)
- "COVID Is Fake Sick Actually Have Influenza A or B", by Dr. Derek KnaussDocumento2 páginas"COVID Is Fake Sick Actually Have Influenza A or B", by Dr. Derek KnaussSANDRA BAGGAinda não há avaliações
- CDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesDocumento7 páginasCDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesAhmad Arbi AninditoAinda não há avaliações
- Pathophys RespDocumento38 páginasPathophys RespSabrina LavegaAinda não há avaliações
- Rle Procedure StudyDocumento4 páginasRle Procedure StudyMyangel LoiseAinda não há avaliações
- Parathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Documento28 páginasParathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Omar Alruwaili100% (1)
- CRF Fluid Volume Excess NCPDocumento3 páginasCRF Fluid Volume Excess NCPchubbielitaAinda não há avaliações
- Patho AsthmaDocumento1 páginaPatho AsthmaAyel JimenezAinda não há avaliações
- Q8Pro POCTDocumento16 páginasQ8Pro POCTSmart BiomedicalAinda não há avaliações
- Personal Health Issues and ConcernDocumento41 páginasPersonal Health Issues and Concernniña pinedaAinda não há avaliações
- Sample Final Exam Questions-f14-KEYDocumento6 páginasSample Final Exam Questions-f14-KEYAlias HedgeAinda não há avaliações
- Digital Covid Questionnaire For Revival Approval FormatDocumento2 páginasDigital Covid Questionnaire For Revival Approval Formatsouravdey3Ainda não há avaliações
- Corona Virus (Covid19) : The Grim RealityDocumento6 páginasCorona Virus (Covid19) : The Grim RealityGenevieve GayosoAinda não há avaliações
- The New Definition and Classification of Seizures and EpilepsyDocumento7 páginasThe New Definition and Classification of Seizures and EpilepsyCarlos Andrés BernalAinda não há avaliações
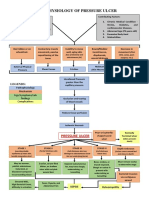
- Pathophysiology of Pressure UlcerDocumento1 páginaPathophysiology of Pressure UlcerSTORAGE FILEAinda não há avaliações
- CHAS Brochure English Jan2014Documento2 páginasCHAS Brochure English Jan2014inabansAinda não há avaliações
- Child Abuse Nursing Care PlansDocumento7 páginasChild Abuse Nursing Care PlansMAHESH KOUJALAGIAinda não há avaliações
- Systematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatDocumento8 páginasSystematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatAdinda Pramesthi RiadyaniAinda não há avaliações
- Immunology and Immunochemistry PDFDocumento8 páginasImmunology and Immunochemistry PDFboatcomAinda não há avaliações
- Faisal Yunus PIPKRA How Adherence To GOLD Improve The COPD Treatment and Economic Outcomes - 3 Feb 2023-1Documento37 páginasFaisal Yunus PIPKRA How Adherence To GOLD Improve The COPD Treatment and Economic Outcomes - 3 Feb 2023-1Muhammad Khairul AfifAinda não há avaliações
- c22 Microbiology Tortora TestbankDocumento16 páginasc22 Microbiology Tortora Testbankwhitewave25Ainda não há avaliações
- Psychiatric ScreeningDocumento1 páginaPsychiatric ScreeningCatalina BorquezAinda não há avaliações
- RetinaDocumento19 páginasRetinaSuze C.Ainda não há avaliações
- Broiler Breeder DiseasesDocumento12 páginasBroiler Breeder DiseasesvetbcasAinda não há avaliações
- Brucellosis Brucellosis: Brucella Spp. Brucella SPPDocumento24 páginasBrucellosis Brucellosis: Brucella Spp. Brucella SPPhussain AltaherAinda não há avaliações
- Hand Hygiene: Panitia Pengendalian Infeksi Nosokomial. Dr. Ahmad D. SudrajatDocumento40 páginasHand Hygiene: Panitia Pengendalian Infeksi Nosokomial. Dr. Ahmad D. SudrajatpedsquadAinda não há avaliações
- Gastro MCQsDocumento14 páginasGastro MCQsvaegmundigAinda não há avaliações
- ClubfootDocumento9 páginasClubfootLorebell100% (5)
- THC AspergerDocumento168 páginasTHC AspergerMICHAELAinda não há avaliações