Você também pode gostar
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesAinda não há avaliações
- Umibilical Cord - ProlapsDocumento22 páginasUmibilical Cord - ProlapsAtikah PurnamasariAinda não há avaliações
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesNo EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesAinda não há avaliações
- CF AdimeDocumento3 páginasCF Adimeapi-302326926Ainda não há avaliações
- Understand Cancer & Reduce Cancer Risk - Based On The Teachings Of Dr. Andrew Huberman: Empowering You To Safeguard Against ItNo EverandUnderstand Cancer & Reduce Cancer Risk - Based On The Teachings Of Dr. Andrew Huberman: Empowering You To Safeguard Against ItAinda não há avaliações
- Diagnosi S: MalariaDocumento28 páginasDiagnosi S: MalariaOm Prakash SinghAinda não há avaliações
- Hand Hygiene Why How and When BrochureDocumento7 páginasHand Hygiene Why How and When BrochureWill JoshAinda não há avaliações
- Normal IntrapartumDocumento42 páginasNormal IntrapartumYemaya84Ainda não há avaliações
- Improving On Sanitation 4Documento9 páginasImproving On Sanitation 4Phamous TayAinda não há avaliações
- Information, Education Communication Aparna AjayDocumento70 páginasInformation, Education Communication Aparna AjayAparna Aby100% (1)
- Nature, Types, Causes and Methods of Abortion: ChapterDocumento38 páginasNature, Types, Causes and Methods of Abortion: ChapterBHUKYA USHARANIAinda não há avaliações
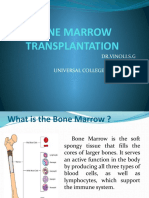
- Bone Marrrow TransplantationDocumento28 páginasBone Marrrow TransplantationvinoliAinda não há avaliações
- BandagingDocumento1 páginaBandagingJescelyn B. CuliananAinda não há avaliações
- Cardiopulmonary ResuscitationDocumento22 páginasCardiopulmonary ResuscitationSundaraBharathiAinda não há avaliações
- E Lert OT LarmedDocumento54 páginasE Lert OT LarmedJetty Elizabeth JoseAinda não há avaliações
- Esophageal CancerDocumento25 páginasEsophageal CancerK poojithaAinda não há avaliações
- Choriocarcinoma 11Documento23 páginasChoriocarcinoma 11Fakhir HasanAinda não há avaliações
- TB MeningitisDocumento17 páginasTB MeningitisSylvan LaminaAinda não há avaliações
- Medico Legal Issues in NursingDocumento17 páginasMedico Legal Issues in Nursingakinyemi loladeAinda não há avaliações
- Pap SmearDocumento3 páginasPap SmearcziehjheyAinda não há avaliações
- Prenatal TestingDocumento26 páginasPrenatal TestingMar ClrAinda não há avaliações
- Surgical Site InfectionDocumento6 páginasSurgical Site InfectionVLSI TECHNOLOGIESAinda não há avaliações
- A Pre Experimental Study To Assess The EDocumento6 páginasA Pre Experimental Study To Assess The ERAMKESH DIWAKARAinda não há avaliações
- Practice Teaching Demonstration: Intracath InsertionDocumento13 páginasPractice Teaching Demonstration: Intracath InsertionMegha lakra100% (1)
- Bone Marrow ChecklistDocumento2 páginasBone Marrow ChecklistHasyim SuparlanAinda não há avaliações
- Warning Signs of Various DiseasesDocumento44 páginasWarning Signs of Various DiseasesamsabavanAinda não há avaliações
- Nursingcaredelivery 181011144230Documento50 páginasNursingcaredelivery 181011144230Nithin RamAinda não há avaliações
- Prevention of Parent To Child Transmission of HIV : Dr. ShobhaDocumento52 páginasPrevention of Parent To Child Transmission of HIV : Dr. ShobhajijaniAinda não há avaliações
- Family Care PlanDocumento5 páginasFamily Care PlanDarwin VillestasAinda não há avaliações
- Care of A Client With: Neonatal Pneumonia: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu CityDocumento22 páginasCare of A Client With: Neonatal Pneumonia: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu CityAsterlyn ConiendoAinda não há avaliações
- Hypertrophic Pyloric StenosisDocumento3 páginasHypertrophic Pyloric StenosisCandice ChengAinda não há avaliações
- A Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotDocumento3 páginasA Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Women &mental HealthDocumento16 páginasWomen &mental HealthDhAiRyA ArOrAAinda não há avaliações
- CervicitisDocumento7 páginasCervicitisElaisa Mae Delos SantosAinda não há avaliações
- Hyper Bilirubin Emi ADocumento29 páginasHyper Bilirubin Emi ANinz NunezAinda não há avaliações
- Patterns of Nursing Care Delivery in IndiaDocumento22 páginasPatterns of Nursing Care Delivery in IndiaBinu JoshvaAinda não há avaliações
- Case Study 2Documento37 páginasCase Study 2api-391842100Ainda não há avaliações
- Epidemilogy Measurment MethodsDocumento100 páginasEpidemilogy Measurment MethodsKailash NagarAinda não há avaliações
- Time Specific Objective Content Teaching Learning Activities Evaluati ONDocumento20 páginasTime Specific Objective Content Teaching Learning Activities Evaluati ONAnnette BainesAinda não há avaliações
- A Topic Presentation ON: Emerging Communicable DiseasesDocumento52 páginasA Topic Presentation ON: Emerging Communicable DiseasesGiri SivaAinda não há avaliações
- Communicable DiseasesDocumento56 páginasCommunicable DiseasesLili Nini100% (1)
- 14 - Professional ResponsibilityDocumento31 páginas14 - Professional ResponsibilityJenish PanchalAinda não há avaliações
- Dengue FeverDocumento5 páginasDengue FeverMae AzoresAinda não há avaliações
- Oxygen Therapy and Oxygen Delivery (Pediatric) - CEDocumento8 páginasOxygen Therapy and Oxygen Delivery (Pediatric) - CEViviana AltamiranoAinda não há avaliações
- Breast Disorders HNII Garner-2 LectureDocumento32 páginasBreast Disorders HNII Garner-2 Lecturesarahbearcoups0% (1)
- Infection Control - LESSON PLANDocumento53 páginasInfection Control - LESSON PLANJincy JohnyAinda não há avaliações
- Assignment On Pharamcological Aspects - BY KAMINI2Documento9 páginasAssignment On Pharamcological Aspects - BY KAMINI2kamini ChoudharyAinda não há avaliações
- Link ClickDocumento4 páginasLink ClickMitch MontielAinda não há avaliações
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDocumento24 páginasNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarAinda não há avaliações
- Cord Care: By: Abella, Wenalyn Grace ZDocumento6 páginasCord Care: By: Abella, Wenalyn Grace ZWenalyn Grace Abella Llavan100% (1)
- Ostomy CareDocumento3 páginasOstomy CareSyamsul ArifinAinda não há avaliações
- History and Physical Assessment of Integumentary System: By: Mr. M - Shiva Nanda ReddyDocumento84 páginasHistory and Physical Assessment of Integumentary System: By: Mr. M - Shiva Nanda ReddyNilakshi Barik MandalAinda não há avaliações
- Nursing Care For HiV Patients Facilitator Guide PDFDocumento314 páginasNursing Care For HiV Patients Facilitator Guide PDFmalathiAinda não há avaliações
- Laryngeal Cancer Powerpoint FinalllllDocumento30 páginasLaryngeal Cancer Powerpoint Finalllllapi-396575125Ainda não há avaliações
- Seminar On Census, National Family Health Survey, Vital StatisticsDocumento18 páginasSeminar On Census, National Family Health Survey, Vital StatisticsANITTA SAinda não há avaliações
- Family Planning Methods - LatestDocumento59 páginasFamily Planning Methods - LatestGenevieve VillaflorAinda não há avaliações
- Updated Operational Guidelines For Mission IndradhanushDocumento76 páginasUpdated Operational Guidelines For Mission IndradhanushZLOOffice BankuraAinda não há avaliações
- Barium Studies: Presented byDocumento18 páginasBarium Studies: Presented byHannah samuelAinda não há avaliações
- Presentation1 Cervical BiopsyDocumento14 páginasPresentation1 Cervical BiopsyChanta MaharjanAinda não há avaliações
- HemorrhoidsDocumento8 páginasHemorrhoidsArt Christian RamosAinda não há avaliações
- Under Graduate Medical Admission Counselling (Ugmac) - 2018 For Mbbs / Bds / Bams / Bhms / BumsDocumento5 páginasUnder Graduate Medical Admission Counselling (Ugmac) - 2018 For Mbbs / Bds / Bams / Bhms / BumschandanAinda não há avaliações
- 113 FullDocumento9 páginas113 FullchandanAinda não há avaliações
- Detailed List of Provisional PensionDocumento1 páginaDetailed List of Provisional PensionchandanAinda não há avaliações
- Kazi Guide Mbbs AnatomyDocumento5 páginasKazi Guide Mbbs Anatomychandan50% (10)
- Is Valid Only With Original Photo IDDocumento2 páginasIs Valid Only With Original Photo IDchandanAinda não há avaliações
- Laplace's Law: What It Is About, Where It Comes From, and How It Is Often Applied in PhysiologyDocumento6 páginasLaplace's Law: What It Is About, Where It Comes From, and How It Is Often Applied in PhysiologychandanAinda não há avaliações
- Behavioral Properties of The Musculotendinous Unit: 1) Extensibility: Ability To Be Stretched or To IncreaseDocumento6 páginasBehavioral Properties of The Musculotendinous Unit: 1) Extensibility: Ability To Be Stretched or To IncreasechandanAinda não há avaliações
- Pre Reg FormsDocumento15 páginasPre Reg FormschandanAinda não há avaliações
- OVERALL CompressedDocumento180 páginasOVERALL CompressedchandanAinda não há avaliações
- What Is Permanent Make-Up?: First in Looks That LastDocumento4 páginasWhat Is Permanent Make-Up?: First in Looks That LastNatural Enhancement0% (1)
- Hemodynamics and Diagnosis Venous Disease-Jvs 1207Documento21 páginasHemodynamics and Diagnosis Venous Disease-Jvs 1207Fahrudin ŠabanovićAinda não há avaliações
- Significance of The Structure of Human SkeletonDocumento5 páginasSignificance of The Structure of Human SkeletonTodirenche LarisaAinda não há avaliações
- Blood Culture Recomendation in PicuDocumento11 páginasBlood Culture Recomendation in PicuJack Eugene LiowAinda não há avaliações
- PancreasDocumento35 páginasPancreasPaskalisAinda não há avaliações
- Medical Imaging and Pattern RecognitionDocumento49 páginasMedical Imaging and Pattern RecognitionworkshoppeAinda não há avaliações
- Barium Swallow (Esophagram) :: Positions and Barium Images PurposeDocumento3 páginasBarium Swallow (Esophagram) :: Positions and Barium Images PurposeAaron SmithAinda não há avaliações
- End-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareDocumento5 páginasEnd-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareSERGIO ANDRES CESPEDES GUERREROAinda não há avaliações
- Essay SamplesDocumento10 páginasEssay SamplesJackie Vacalares100% (1)
- Clark IndigestionDocumento50 páginasClark IndigestionRaveendra MungaraAinda não há avaliações
- Acute GastroenteritisDocumento56 páginasAcute Gastroenteritisneil052298% (46)
- WP Content Uploads 2014 03 Practice Question Set On Reasoning For Ibps Probationary Officer Exam 2012 Freshers AddaDocumento22 páginasWP Content Uploads 2014 03 Practice Question Set On Reasoning For Ibps Probationary Officer Exam 2012 Freshers AddaPaavni SharmaAinda não há avaliações
- Psycho-Oncology - The 6 Phases of Cancer EbookDocumento101 páginasPsycho-Oncology - The 6 Phases of Cancer EbookAndré Amorim100% (2)
- The Scoring Clinical Index For OnychomycosisDocumento4 páginasThe Scoring Clinical Index For OnychomycosisPatricia Avalos C.Ainda não há avaliações
- Non-Alcoholic Fatty Liver DiseaseDocumento15 páginasNon-Alcoholic Fatty Liver DiseaseKurnia pralisaAinda não há avaliações
- Art Theraphy AutismDocumento2 páginasArt Theraphy AutismMatheaFiliAinda não há avaliações
- Asperger Syndrome in ChildrenDocumento8 páginasAsperger Syndrome in Childrenmaria_kazaAinda não há avaliações
- CostIt-example (Primary Health Care Facility)Documento69 páginasCostIt-example (Primary Health Care Facility)Parimalakrishnan100% (1)
- Scripta Medica Volume 44 Issue 1Documento68 páginasScripta Medica Volume 44 Issue 1Zdravko GrubacAinda não há avaliações
- AbtVitalsilRe MushroomDocumento2 páginasAbtVitalsilRe Mushroommds9216Ainda não há avaliações
- Course NotesDocumento125 páginasCourse Notesfuji_reihAinda não há avaliações
- Spice Wise ProductionDocumento2 páginasSpice Wise ProductionMohd IqbalAinda não há avaliações
- Surving Sepsis Campaign ResultDocumento8 páginasSurving Sepsis Campaign Resultmaria arenas de itaAinda não há avaliações
- Measurement ScalesDocumento6 páginasMeasurement ScalesRohit PandeyAinda não há avaliações
- Cardiopulmonary Resuscitation Clinical Skill ChecklistDocumento2 páginasCardiopulmonary Resuscitation Clinical Skill ChecklistCarissa TirtaniaAinda não há avaliações
- No-Scar Transoral Thyroglossal Duct Cyst Excision in ChildrenDocumento21 páginasNo-Scar Transoral Thyroglossal Duct Cyst Excision in ChildrenMishel Rodriguez GuzmanAinda não há avaliações
- Typhoid FeverDocumento46 páginasTyphoid Feverdeskichinta50% (2)
- Renal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyDocumento50 páginasRenal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyMarivic DianoAinda não há avaliações
- Capstone OutlineDocumento3 páginasCapstone Outlineapi-395468231Ainda não há avaliações
- Cell Wall Inhibitor PPT SlideDocumento47 páginasCell Wall Inhibitor PPT Slidekhawaja sahabAinda não há avaliações
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeAinda não há avaliações
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayNo EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayNota: 4.5 de 5 estrelas4.5/5 (3)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeNo EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeNota: 3.5 de 5 estrelas3.5/5 (13)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouAinda não há avaliações
- What to Expect When You’re Expecting (5th Edition)No EverandWhat to Expect When You’re Expecting (5th Edition)Nota: 5 de 5 estrelas5/5 (1)
- Skinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!No EverandSkinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!Nota: 3.5 de 5 estrelas3.5/5 (489)
- Awakening Fertility: The Essential Art of Preparing for PregnancyNo EverandAwakening Fertility: The Essential Art of Preparing for PregnancyNota: 4.5 de 5 estrelas4.5/5 (36)
- Intoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingNo EverandIntoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingNota: 5 de 5 estrelas5/5 (1)
- Natural Hospital Birth: The Best of Both WorldsNo EverandNatural Hospital Birth: The Best of Both WorldsNota: 5 de 5 estrelas5/5 (33)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisNo EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisNota: 3 de 5 estrelas3/5 (2)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondNo EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondNota: 4.5 de 5 estrelas4.5/5 (39)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenNo EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenNota: 4 de 5 estrelas4/5 (154)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersNo EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersNota: 4.5 de 5 estrelas4.5/5 (72)
- Pregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!No EverandPregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Nota: 5 de 5 estrelas5/5 (1)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodNo EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodNota: 5 de 5 estrelas5/5 (33)
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondNo EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondNota: 4 de 5 estrelas4/5 (111)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouNo EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouNota: 4 de 5 estrelas4/5 (25)
- Reclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeNo EverandReclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeNota: 5 de 5 estrelas5/5 (16)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.No EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Nota: 4.5 de 5 estrelas4.5/5 (124)
- Crones Don't Whine: Concentrated Wisdom for Juicy WomenNo EverandCrones Don't Whine: Concentrated Wisdom for Juicy WomenNota: 2.5 de 5 estrelas2.5/5 (3)
- The Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysNo EverandThe Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysNota: 4.5 de 5 estrelas4.5/5 (5)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionNo EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionNota: 4.5 de 5 estrelas4.5/5 (125)
- The Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityNo EverandThe Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityNota: 4.5 de 5 estrelas4.5/5 (12)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondNo EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondNota: 4.5 de 5 estrelas4.5/5 (3)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainNo EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainNota: 4 de 5 estrelas4/5 (14)
- Period Repair Manual: Natural Treatment for Better Hormones and Better Periods, 2nd editionNo EverandPeriod Repair Manual: Natural Treatment for Better Hormones and Better Periods, 2nd editionNota: 4.5 de 5 estrelas4.5/5 (28)
- Real Food for Mother and Baby: The Fertility Diet, Eating for Two, and Baby's First FoodsNo EverandReal Food for Mother and Baby: The Fertility Diet, Eating for Two, and Baby's First FoodsNota: 4 de 5 estrelas4/5 (19)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.No EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Nota: 3.5 de 5 estrelas3.5/5 (7)