Você também pode gostar
- HVLV Map - SEQ 236752603Documento10 páginasHVLV Map - SEQ 236752603ranafaraz009Ainda não há avaliações
- Chapter 11 - Motivating and Rewarding EmployeesDocumento19 páginasChapter 11 - Motivating and Rewarding EmployeesJadulco, Joris Jezreel V.Ainda não há avaliações
- NC PresentationDocumento20 páginasNC PresentationwahyudiAinda não há avaliações
- Coursera Computer Network Certificate Cse 307 PDFDocumento1 páginaCoursera Computer Network Certificate Cse 307 PDFstacyAinda não há avaliações
- G74 KSK 60236Documento1 páginaG74 KSK 60236Ashkan AsefiAinda não há avaliações
- Myths of Dental Surgery in Patients Receiving Anticoagulant PDFDocumento6 páginasMyths of Dental Surgery in Patients Receiving Anticoagulant PDFAlexandra MartinezAinda não há avaliações
- Handbook-RefrigerationDocumento67 páginasHandbook-RefrigerationDDCMAinda não há avaliações
- 20 Years of Zebra & Quagga Mussel Research at NOAA's Great Lakes Environmental Research LaboratoryDocumento2 páginas20 Years of Zebra & Quagga Mussel Research at NOAA's Great Lakes Environmental Research LaboratoryGreat Lakes Environmental Research LaboratoryAinda não há avaliações
- National Climbing Rappelling Safety Standards (1) - CompressedDocumento4 páginasNational Climbing Rappelling Safety Standards (1) - CompressedYDread OfficialAinda não há avaliações
- Faculty of Engineering, Technology Applied Design and Fine ArtDocumento48 páginasFaculty of Engineering, Technology Applied Design and Fine Artmuhammedssebatindira3Ainda não há avaliações
- G71 KSK 60236Documento1 páginaG71 KSK 60236Ashkan AsefiAinda não há avaliações
- An Updated Review of Hypertensive Emergencies and Urgencies: Katalin Makó, Corina Ureche, Zsuzsanna JeremiásDocumento11 páginasAn Updated Review of Hypertensive Emergencies and Urgencies: Katalin Makó, Corina Ureche, Zsuzsanna JeremiásiganuryantiAinda não há avaliações
- TriggerDocumento3 páginasTriggerarchana pradhanAinda não há avaliações
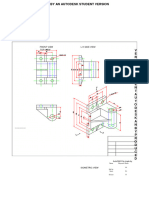
- Graphics MayureshDocumento2 páginasGraphics Mayureshsunitaraje16Ainda não há avaliações
- 01-Air BersihDocumento1 página01-Air Bersihk3 rsuihaAinda não há avaliações
- Part Number: H001Ssc800 Description: Forester PND Navi. Audio UnitDocumento21 páginasPart Number: H001Ssc800 Description: Forester PND Navi. Audio UnitKavita Jha100% (1)
- Hell Hades Faction Wars GuideDocumento14 páginasHell Hades Faction Wars GuidepiloframiAinda não há avaliações
- Data Flow Chart - 2Documento2 páginasData Flow Chart - 2shaik sameeruddinAinda não há avaliações
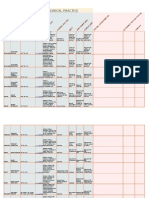
- Goniometry For Clinical PracticeDocumento7 páginasGoniometry For Clinical Practicedramitsaini33% (3)
- 7 Caves 22+500-22+700 RW - 1Documento1 página7 Caves 22+500-22+700 RW - 14jhe Di4sAinda não há avaliações
- Cross Section STA.22+540 CS/ 3 OF 12: Republica Democratica de Timor LesteDocumento1 páginaCross Section STA.22+540 CS/ 3 OF 12: Republica Democratica de Timor Leste4jhe Di4sAinda não há avaliações
- Cross Section STA.22+560 CS/ 4 OF 12: Republica Democratica de Timor LesteDocumento1 páginaCross Section STA.22+560 CS/ 4 OF 12: Republica Democratica de Timor Leste4jhe Di4sAinda não há avaliações
- Lplpo Dak, Apbn, Dak 2019 DLL NTDocumento18 páginasLplpo Dak, Apbn, Dak 2019 DLL NTovhynAinda não há avaliações
- Planteamiento-Perfiles y CortesDocumento1 páginaPlanteamiento-Perfiles y CortesJefferson Auqui OtarolaAinda não há avaliações
- MCH418/MCH618: Four Post/Six Post Mobile Column Lift 24V DC PoweredDocumento16 páginasMCH418/MCH618: Four Post/Six Post Mobile Column Lift 24V DC Poweredניקולאי איןAinda não há avaliações
- Professions and Applications of GeomaticsDocumento33 páginasProfessions and Applications of GeomaticsHazel RiyenziAinda não há avaliações
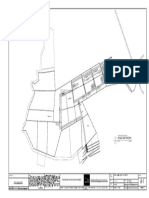
- Existing Contour and Site LayoutDocumento1 páginaExisting Contour and Site LayoutAlexander MasongsongAinda não há avaliações
- Road Network: Proposed Bataan DevelopmentDocumento1 páginaRoad Network: Proposed Bataan DevelopmentJigo AlianganAinda não há avaliações
- BI-10-09004-0004 Marjan Increment Program Jubail Area-Pipeline Projact PKG#18 DC System Sizing CalculationDocumento32 páginasBI-10-09004-0004 Marjan Increment Program Jubail Area-Pipeline Projact PKG#18 DC System Sizing CalculationAfzal AsifAinda não há avaliações
- Annual Goal StrengthenningDocumento3 páginasAnnual Goal StrengthenninglyspichhAinda não há avaliações
- CONJUNTODocumento1 páginaCONJUNTOAbigail RuízAinda não há avaliações
- 2017 GINA Report, Global Strategy For Asthma Management and Prevention PDFDocumento159 páginas2017 GINA Report, Global Strategy For Asthma Management and Prevention PDFNalemi JT100% (1)
- Cavallaro2011 REPORTE DE IMPLANTE ANGULADODocumento9 páginasCavallaro2011 REPORTE DE IMPLANTE ANGULADOXiomara Reyes palominoAinda não há avaliações
- Curvas de NivelDocumento1 páginaCurvas de Nivellucho champi quispeAinda não há avaliações
- Wms GINA 2018 Strategy Report V1.1 PDFDocumento161 páginasWms GINA 2018 Strategy Report V1.1 PDFEdson ArmandoAinda não há avaliações
- Cuest DiscriminaiónJADA2010Documento9 páginasCuest DiscriminaiónJADA2010Miguel Walter Ramón NeyraAinda não há avaliações
- Learning and Development Best PracticeDocumento20 páginasLearning and Development Best PracticeshalinivaAinda não há avaliações
- Hand Rendered Sketch PDFDocumento1 páginaHand Rendered Sketch PDFShruti JhaAinda não há avaliações
- Chapter 1 Part2Documento29 páginasChapter 1 Part2刘伟康Ainda não há avaliações
- Gestión Interna de Residuos y Desechos Generados en Establecimientos de Salud 2023. - CertificadoDocumento1 páginaGestión Interna de Residuos y Desechos Generados en Establecimientos de Salud 2023. - CertificadoDE CERO A PREZIAinda não há avaliações
- Religion of Ancient EgyptDocumento3 páginasReligion of Ancient EgyptDania UsmamAinda não há avaliações
- Treating Obstructive Sleep Apnea and Snoring: Assessment of An Anterior Mandibular Positioning DeviceDocumento7 páginasTreating Obstructive Sleep Apnea and Snoring: Assessment of An Anterior Mandibular Positioning Device陈延珑Ainda não há avaliações
- v14n3 PDFDocumento32 páginasv14n3 PDFELENAinda não há avaliações
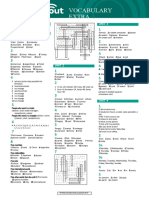
- Speakout Vocabulary Extra Starter Answer Key (11 Files Merged)Documento23 páginasSpeakout Vocabulary Extra Starter Answer Key (11 Files Merged)Carlos JorgeAinda não há avaliações
- Old Aberdeen Campus MapDocumento1 páginaOld Aberdeen Campus MapAdrian Arturo Hernandez RosalesAinda não há avaliações
- Submittal Data Information: TC Series Pumps (60 HZ NEMA)Documento2 páginasSubmittal Data Information: TC Series Pumps (60 HZ NEMA)Bagaskoro Dwi PrastioAinda não há avaliações
- Profile: ISO 17025, NABL Accredited Lab Cert. No.: T-0197 & T-0198Documento12 páginasProfile: ISO 17025, NABL Accredited Lab Cert. No.: T-0197 & T-0198RB SinghAinda não há avaliações
- Gantt Chart NewDocumento9 páginasGantt Chart NewpokjatAinda não há avaliações
- IMvula Quality Protection ProfileDocumento33 páginasIMvula Quality Protection ProfileAnonymous fSKAwNCAinda não há avaliações
- Creating Videos With Confidence WorkbookDocumento29 páginasCreating Videos With Confidence Workbookvero baudensAinda não há avaliações
- FILIPO CompressedDocumento1 páginaFILIPO CompressedCarolina CarrascoAinda não há avaliações
- Dia VW J VK/KKFJR Ijh (KK Ds Fy, Ço'S K IDocumento5 páginasDia VW J VK/KKFJR Ijh (KK Ds Fy, Ço'S K IShanmuga RajaAinda não há avaliações
- Belimed - CA 9600 Sell Sheet - 08 2016Documento2 páginasBelimed - CA 9600 Sell Sheet - 08 2016Icee SinlapasertAinda não há avaliações
- Financial Forecasts and Determination of Financial Feasibility BTLED STUDDocumento23 páginasFinancial Forecasts and Determination of Financial Feasibility BTLED STUDjared catanguiAinda não há avaliações
- See Hss Base Plate Detail: 5 8 3 4 5 8 3 8 1 4 Scale: 1 "-1'-0"Documento1 páginaSee Hss Base Plate Detail: 5 8 3 4 5 8 3 8 1 4 Scale: 1 "-1'-0"James PittsAinda não há avaliações
- Oman Daily ObserverDocumento28 páginasOman Daily ObserverAnil KumarAinda não há avaliações
- Kirsch Douglas - Whats Your Number - Diagnosing Obstructive Sleep Apnea in 2019 PDFDocumento15 páginasKirsch Douglas - Whats Your Number - Diagnosing Obstructive Sleep Apnea in 2019 PDFCaioSelaimenAinda não há avaliações
- The Link Between Sleep Bruxism, Sleep Disordered Breathing and Temporomandibular Disorders: An Evidence-Based ReviewDocumento11 páginasThe Link Between Sleep Bruxism, Sleep Disordered Breathing and Temporomandibular Disorders: An Evidence-Based ReviewCaioSelaimenAinda não há avaliações
- De Leeuw RDocumento14 páginasDe Leeuw RCaioSelaimenAinda não há avaliações
- Fasc Dor OrofacialDocumento5 páginasFasc Dor OrofacialCaioSelaimenAinda não há avaliações
- 2016 Article 653Documento20 páginas2016 Article 653CaioSelaimenAinda não há avaliações
- Botulinum Toxin Therapy For Temporomandibular Joint Disorders: A Systematic Review of Randomized Controlled TrialsDocumento9 páginasBotulinum Toxin Therapy For Temporomandibular Joint Disorders: A Systematic Review of Randomized Controlled TrialsCaioSelaimenAinda não há avaliações
- 1 s2.0 S0901502715001782 MainDocumento7 páginas1 s2.0 S0901502715001782 MainCaioSelaimenAinda não há avaliações
- Assessment of Bruxism in The Clinic PDFDocumento14 páginasAssessment of Bruxism in The Clinic PDFCaioSelaimenAinda não há avaliações
- Eb Mmo4106Documento16 páginasEb Mmo4106CaioSelaimen100% (2)
- 5509 19744 1 PBDocumento5 páginas5509 19744 1 PBCaioSelaimenAinda não há avaliações
- Potsdam Village Police Dept. Blotter Sept. 10, 2017Documento2 páginasPotsdam Village Police Dept. Blotter Sept. 10, 2017NewzjunkyAinda não há avaliações
- Tetanus - AnatomyDocumento7 páginasTetanus - AnatomyJoro27Ainda não há avaliações
- Women Devlopment-Government Policies and ProgrammesDocumento19 páginasWomen Devlopment-Government Policies and ProgrammesVishalMishraAinda não há avaliações
- QUARTER 3 WEEK 3 English For Academic and PPDocumento11 páginasQUARTER 3 WEEK 3 English For Academic and PPCharmaine PearlAinda não há avaliações
- Intermittent Positive Pressure BreathingDocumento12 páginasIntermittent Positive Pressure BreathingHitesh RohitAinda não há avaliações
- Combat StressDocumento94 páginasCombat StressClaudia Maria Ivan100% (1)
- Seminar and Topic ObjectivesDocumento2 páginasSeminar and Topic ObjectivesNeyo KatalbasAinda não há avaliações
- Form Lplpo Pustu Dan PoskesdesDocumento3 páginasForm Lplpo Pustu Dan PoskesdesristiAinda não há avaliações
- Mangune v. Ermita (2016)Documento3 páginasMangune v. Ermita (2016)Cristelle Elaine Collera100% (1)
- Written Assignment Unit 2 - HS 2212Documento5 páginasWritten Assignment Unit 2 - HS 2212bnvjAinda não há avaliações
- SIPDocumento2 páginasSIPRowena Abdula BaronaAinda não há avaliações
- Zombie Brains PDFDocumento1 páginaZombie Brains PDFLorna GrayAinda não há avaliações
- Superficial FatsDocumento29 páginasSuperficial FatsCatalina Soler LioiAinda não há avaliações
- Nzmail 18821014Documento26 páginasNzmail 18821014zeljkogrAinda não há avaliações
- Strengthening Health Emergency Management System Through The ILHZDocumento7 páginasStrengthening Health Emergency Management System Through The ILHZCliff GubatAinda não há avaliações
- CircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesDocumento43 páginasCircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesMenaAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar PustakaNi Made Ayu DwipayantiAinda não há avaliações
- Health Beliefs and PracticesDocumento7 páginasHealth Beliefs and Practicesapi-283426681Ainda não há avaliações
- Lecture #3 - Carbohydrates & LipidsDocumento23 páginasLecture #3 - Carbohydrates & Lipidsogangurel100% (3)
- VE4 Sem 1 Student Packet (25 July)Documento187 páginasVE4 Sem 1 Student Packet (25 July)Dwayne June GetiganAinda não há avaliações
- NCP For PostpartumDocumento1 páginaNCP For PostpartumMary Hope BacutaAinda não há avaliações
- Week 4.1 The Law of ResonanceDocumento12 páginasWeek 4.1 The Law of ResonanceWim Massop100% (1)
- Chapter I Related Literature Teenage PreDocumento12 páginasChapter I Related Literature Teenage PreWilkenn Tuazon100% (3)
- ABO Blood GroupDocumento12 páginasABO Blood GroupGhost AnkanAinda não há avaliações
- Labor and Delivery OB Concept MapDocumento2 páginasLabor and Delivery OB Concept MapMissy Johnson75% (4)
- 21.JMM Promotion and Management, Inc. vs. Court of AppealsDocumento3 páginas21.JMM Promotion and Management, Inc. vs. Court of AppealsnathAinda não há avaliações
- 3M Disposable Filtering Facepiece Respirator Fitting Poster English and SpanishDocumento2 páginas3M Disposable Filtering Facepiece Respirator Fitting Poster English and SpanishTrunggana AbdulAinda não há avaliações
- The Rating Scale Is As FollowsDocumento3 páginasThe Rating Scale Is As Followscarollim1008Ainda não há avaliações
- Experiment 9 - Hydrolysis of CarbohydratesDocumento2 páginasExperiment 9 - Hydrolysis of CarbohydratesJuren LasagaAinda não há avaliações
- Official ResumeDocumento1 páginaOfficial ResumeBrianna DallalAinda não há avaliações
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainNo EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainNota: 4 de 5 estrelas4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNota: 4 de 5 estrelas4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (59)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (45)