Você também pode gostar
- FNCP Hypertension 1Documento2 páginasFNCP Hypertension 1revita lestariAinda não há avaliações
- Jurnal 6Documento13 páginasJurnal 6dewi pspta sriAinda não há avaliações
- ContentServer 3Documento8 páginasContentServer 3Riris KurnialatriAinda não há avaliações
- Stigma and Outcome of Treatment Among Patients With Psychological Disorders and Their AttendersDocumento5 páginasStigma and Outcome of Treatment Among Patients With Psychological Disorders and Their AttendersFathima ZoharaAinda não há avaliações
- Anti Stigma TaiwanDocumento8 páginasAnti Stigma TaiwanLeticia Raquel Pe�a Pe�aAinda não há avaliações
- Indian J Psychiatry Skizo Impact On QoLDocumento12 páginasIndian J Psychiatry Skizo Impact On QoLAnonymous hvOuCjAinda não há avaliações
- Efficacy of Psychological Intervention For Patients With Psoriasis Vulgaris: A Prospective StudyDocumento8 páginasEfficacy of Psychological Intervention For Patients With Psoriasis Vulgaris: A Prospective StudyTeuku FadhliAinda não há avaliações
- Author's Accepted Manuscript: Psychiatry ResearchDocumento24 páginasAuthor's Accepted Manuscript: Psychiatry ResearchbadrulAinda não há avaliações
- Mental HealthDocumento8 páginasMental HealthJohn TelekAinda não há avaliações
- Ser 9 3 240Documento8 páginasSer 9 3 240Catarina C.Ainda não há avaliações
- Quality of Life in Caregivers of Patients With Schizophrenia A Literature ReviewDocumento6 páginasQuality of Life in Caregivers of Patients With Schizophrenia A Literature Reviewgw0q12dxAinda não há avaliações
- Subjective and Objective Caregiver Burden in Parkinson's DiseaseDocumento7 páginasSubjective and Objective Caregiver Burden in Parkinson's Diseasearpit11111Ainda não há avaliações
- Effects of The Nursing Psychoeducation Program On The Acceptance of Medication and Condition-Specific Knowledge of PatientDocumento6 páginasEffects of The Nursing Psychoeducation Program On The Acceptance of Medication and Condition-Specific Knowledge of PatientEric KatškovskiAinda não há avaliações
- 1 s2.0 S0883941722000905 MainDocumento11 páginas1 s2.0 S0883941722000905 MainReni Tri AstutiAinda não há avaliações
- Diff Erences in Cognitive Function and Daily Living Skills Between Early-And Late-Stage SchizophreniaDocumento8 páginasDiff Erences in Cognitive Function and Daily Living Skills Between Early-And Late-Stage SchizophreniaRenny TjahjaAinda não há avaliações
- Archives of Psychiatric Nursing: Lora Humphrey Beebe, Kathleen Smith, Chad PhillipsDocumento6 páginasArchives of Psychiatric Nursing: Lora Humphrey Beebe, Kathleen Smith, Chad PhillipsArif IrpanAinda não há avaliações
- Ijepr MarchDocumento6 páginasIjepr MarchnandhaAinda não há avaliações
- Journal Presentation: By, R.Angelin Thangam Bot Final YearDocumento50 páginasJournal Presentation: By, R.Angelin Thangam Bot Final YearAarthi ArumugamAinda não há avaliações
- Vassetal 2015Documento9 páginasVassetal 2015njevkoAinda não há avaliações
- Factor Structure Analysis, Validity and Reliability of The Health Anxiety Inventory-Short FormDocumento7 páginasFactor Structure Analysis, Validity and Reliability of The Health Anxiety Inventory-Short FormDenisa IonașcuAinda não há avaliações
- Hanza Wa 2013Documento6 páginasHanza Wa 2013MicciAinda não há avaliações
- Descriptive StatisticsDocumento16 páginasDescriptive StatisticsSaadia TalibAinda não há avaliações
- Vass 2015Documento9 páginasVass 2015Amina LabiadhAinda não há avaliações
- Take Charge Personality As Predictor of Recovery From Eating DisorderDocumento6 páginasTake Charge Personality As Predictor of Recovery From Eating DisorderRokas JonasAinda não há avaliações
- Bodily and Austin Final DraftDocumento29 páginasBodily and Austin Final Draftapi-582011343Ainda não há avaliações
- Occupational Therapy For Inpatients With Chronic Schizophrenia: A Pilot Randomized Controlled TrialDocumento6 páginasOccupational Therapy For Inpatients With Chronic Schizophrenia: A Pilot Randomized Controlled TrialAngela EnacheAinda não há avaliações
- Exploring Risk Factors For Depression Among Older Men Residing in MacauDocumento11 páginasExploring Risk Factors For Depression Among Older Men Residing in MacauaryaAinda não há avaliações
- QOL CopingDocumento10 páginasQOL CopingNisa PradityaAinda não há avaliações
- 1 s2.0 S0165178112006397 MainDocumento6 páginas1 s2.0 S0165178112006397 Mainirene de la cuestaAinda não há avaliações
- Insight, Self-Stigma and PsychosociaDocumento10 páginasInsight, Self-Stigma and PsychosociaJana AlvesAinda não há avaliações
- 08.06.09 - Psychosocial Impact of Dysthymia A Study Among Married PatientsDocumento6 páginas08.06.09 - Psychosocial Impact of Dysthymia A Study Among Married PatientsRiham AmmarAinda não há avaliações
- Epilepsy & Behavior: Shanna M. Guilfoyle, Sally Monahan, Cindy Wesolowski, Avani C. ModiDocumento6 páginasEpilepsy & Behavior: Shanna M. Guilfoyle, Sally Monahan, Cindy Wesolowski, Avani C. ModiJhonny BatongAinda não há avaliações
- Mond 2010klkoojljljlDocumento20 páginasMond 2010klkoojljljlverghese17Ainda não há avaliações
- Adverse Effects of Perceived Stigma On Social Adaptation of Persons Diagnosed With Bipolar Affective DisorderDocumento6 páginasAdverse Effects of Perceived Stigma On Social Adaptation of Persons Diagnosed With Bipolar Affective Disordershah khalidAinda não há avaliações
- Associations of Physical Activity, Screen Time With Depression, Anxiety and Sleep Quality Among Chinese College FreshmenDocumento5 páginasAssociations of Physical Activity, Screen Time With Depression, Anxiety and Sleep Quality Among Chinese College FreshmenReynaldy Anggara SaputraAinda não há avaliações
- KIneski Rad StigmaDocumento8 páginasKIneski Rad StigmanjevkoAinda não há avaliações
- Research Article: Stresses and Disability in Depression Across GenderDocumento9 páginasResearch Article: Stresses and Disability in Depression Across GenderWaleed RehmanAinda não há avaliações
- Correlates of General Quality of Life Are Different in Patients With Primary Insomnia As Compared To Patients With Insomnia and Psychiatric ComorbidityDocumento13 páginasCorrelates of General Quality of Life Are Different in Patients With Primary Insomnia As Compared To Patients With Insomnia and Psychiatric ComorbidityVictor CarrenoAinda não há avaliações
- The Impact of Multidisciplinary Rehabilitation On The Quality of Life of Hemodialysis Patients in IranDocumento7 páginasThe Impact of Multidisciplinary Rehabilitation On The Quality of Life of Hemodialysis Patients in IranDewi KusumastutiAinda não há avaliações
- NIH Public AccessDocumento15 páginasNIH Public AccessSofía SciglianoAinda não há avaliações
- Insight and Symptom Severity in An Inpatient Psychiatric SampleDocumento12 páginasInsight and Symptom Severity in An Inpatient Psychiatric SamplealejandraAinda não há avaliações
- Shukla-Rishi2018 Article HealthLocusOfControlPsychosociDocumento8 páginasShukla-Rishi2018 Article HealthLocusOfControlPsychosociMarie McFressieAinda não há avaliações
- Long-Term Follow-Up Ofthe Tips Early Detection in Psychosisstudy:Effectson 10-YearoutcomeDocumento7 páginasLong-Term Follow-Up Ofthe Tips Early Detection in Psychosisstudy:Effectson 10-YearoutcomeELvine GunawanAinda não há avaliações
- WilianDocumento8 páginasWilianĐỗ Văn ĐứcAinda não há avaliações
- LR EthicsDocumento3 páginasLR EthicsUsman DostAinda não há avaliações
- A Systematic Review and Psychometric Evaluation of Self-Report HoardingDocumento45 páginasA Systematic Review and Psychometric Evaluation of Self-Report HoardingAmita GoyalAinda não há avaliações
- 1 s2.0 S0022395622000103 MainDocumento9 páginas1 s2.0 S0022395622000103 MainFachry RahmanAinda não há avaliações
- Occupational Therapy and Mental Health 1Documento18 páginasOccupational Therapy and Mental Health 1Roman -Ainda não há avaliações
- Ijerph 18 04746Documento10 páginasIjerph 18 04746Arif IrpanAinda não há avaliações
- Multiple Outcome Parameters: A 10 Year Follow-Up Study of First-Episode SchizophreniaDocumento7 páginasMultiple Outcome Parameters: A 10 Year Follow-Up Study of First-Episode SchizophreniadianaAinda não há avaliações
- Manuscrip 2 PDFDocumento41 páginasManuscrip 2 PDFayu purnamaAinda não há avaliações
- Recurrent MiscarriageDocumento5 páginasRecurrent MiscarriagedindaAinda não há avaliações
- Guia EsquizoDocumento8 páginasGuia EsquizoSeleccion PersonalAinda não há avaliações
- Cambios de Personalidad y Personalidad Como Predictor Del Cambio en PsicoterapiaDocumento23 páginasCambios de Personalidad y Personalidad Como Predictor Del Cambio en PsicoterapiaLaboratorio CuantiAinda não há avaliações
- The Factors Associated With Depression in Schizophrenia Patients: The Role of Self-Efficacy, Self-Esteem, Hope and ResilienceDocumento14 páginasThe Factors Associated With Depression in Schizophrenia Patients: The Role of Self-Efficacy, Self-Esteem, Hope and ResilienceArif IrpanAinda não há avaliações
- Family Interventions For Bipolar DisorderDocumento3 páginasFamily Interventions For Bipolar DisorderRanda NurawiAinda não há avaliações
- The Impact of Infertility On The Psychological Well-Being, Marital Relationships, Sexual Relationships, and Quality of Life of Couples: A Systematic ReviewDocumento17 páginasThe Impact of Infertility On The Psychological Well-Being, Marital Relationships, Sexual Relationships, and Quality of Life of Couples: A Systematic ReviewAnaAinda não há avaliações
- 01 Taylor-Rodgers Evaluation of An Online 2014Documento7 páginas01 Taylor-Rodgers Evaluation of An Online 2014sushmita bhartiaAinda não há avaliações
- Cultivating Empathy For The Mentally Ill Using Simulated Auditory HallucinationsDocumento4 páginasCultivating Empathy For The Mentally Ill Using Simulated Auditory HallucinationsGloria Carbajal ZegarraAinda não há avaliações
- Asian Journal of Psychiatry: Vijeta Kushwaha, Koushik Sinha Deb, Rakesh K. Chadda, Manju MehtaDocumento3 páginasAsian Journal of Psychiatry: Vijeta Kushwaha, Koushik Sinha Deb, Rakesh K. Chadda, Manju MehtaLaumart HukomAinda não há avaliações
- Hearing Voices: Qualitative Inquiry in Early PsychosisNo EverandHearing Voices: Qualitative Inquiry in Early PsychosisAinda não há avaliações
- Nihms 463562Documento16 páginasNihms 463562windaRQ96Ainda não há avaliações
- Feeding of Infants and Young Children in Tsunami Affected Villages in PondicherryDocumento4 páginasFeeding of Infants and Young Children in Tsunami Affected Villages in PondicherrywindaRQ96Ainda não há avaliações
- Ijerph 09 03384Documento14 páginasIjerph 09 03384windaRQ96Ainda não há avaliações
- Adhesive Capsulitis of The Shoulder and Diabetes: A Meta-Analysis of PrevalenceDocumento9 páginasAdhesive Capsulitis of The Shoulder and Diabetes: A Meta-Analysis of PrevalencewindaRQ96Ainda não há avaliações
- NIH Public Access: Author ManuscriptDocumento18 páginasNIH Public Access: Author ManuscriptwindaRQ96Ainda não há avaliações
- Afhs0501 0004 PDFDocumento10 páginasAfhs0501 0004 PDFwindaRQ96Ainda não há avaliações
- Group Medical Visits (GMVS) in Primary Care: An RCT of Group-Based Versus Individual Appointments To Reduce Hba1C in Older PeopleDocumento10 páginasGroup Medical Visits (GMVS) in Primary Care: An RCT of Group-Based Versus Individual Appointments To Reduce Hba1C in Older PeoplewindaRQ96Ainda não há avaliações
- Dr. Lamia El Wakeel, PhD. Lecturer of Clinical Pharmacy Ain Shams UniversityDocumento19 páginasDr. Lamia El Wakeel, PhD. Lecturer of Clinical Pharmacy Ain Shams UniversitysamvetAinda não há avaliações
- Sickle-Cell AnemiaDocumento11 páginasSickle-Cell Anemiahalzen_joyAinda não há avaliações
- Care Plan - Chronic PainDocumento4 páginasCare Plan - Chronic Painapi-246639896Ainda não há avaliações
- Ethics Uworld NotesDocumento3 páginasEthics Uworld NotesActeen MyoseenAinda não há avaliações
- Acute Iron Poisoning - PharmacologyDocumento10 páginasAcute Iron Poisoning - PharmacologyAmmaarah IsaacsAinda não há avaliações
- Agent CharacteristicsDocumento2 páginasAgent Characteristicsyiaili1234100% (1)
- Reproductive Tract InfectionDocumento48 páginasReproductive Tract InfectionSampriti Roy100% (1)
- Cue and Clue Problem List and Initial Diagnosis PlanningDocumento3 páginasCue and Clue Problem List and Initial Diagnosis PlanningWilujeng AnggrainiAinda não há avaliações
- AWES Question Papers For Home ScienceDocumento5 páginasAWES Question Papers For Home ScienceAtul SharmaAinda não há avaliações
- Index Case Presentation: TuberculosisDocumento14 páginasIndex Case Presentation: Tuberculosisnandini singhAinda não há avaliações
- ADA Cal en DT ADS001150 Rev01Documento1 páginaADA Cal en DT ADS001150 Rev01vijayramaswamyAinda não há avaliações
- Pathophysiology of HypertensionDocumento54 páginasPathophysiology of HypertensionKaloy Kamao100% (3)
- Low Blood Pressure (Hypotension) Lifestyle Mayo ClinicDocumento8 páginasLow Blood Pressure (Hypotension) Lifestyle Mayo ClinicanupamrcAinda não há avaliações
- RPHC4004 Fashion Constructed Image: AgoraphobiaDocumento51 páginasRPHC4004 Fashion Constructed Image: Agoraphobiacstanhope01Ainda não há avaliações
- Evaluation and Management of Shock States: Hypovolemic, Distributive, and Cardiogenic ShockDocumento17 páginasEvaluation and Management of Shock States: Hypovolemic, Distributive, and Cardiogenic ShockMarest AskynaAinda não há avaliações
- Hypersensitivity ReactionsDocumento12 páginasHypersensitivity Reactionsella Sy100% (1)
- k.21 Dry PleurisyDocumento14 páginask.21 Dry PleurisyWinson ChitraAinda não há avaliações
- Using and Interpreting Stressscan: Envisia Learning 3435 Ocean Park BLVD, Suite 203Documento64 páginasUsing and Interpreting Stressscan: Envisia Learning 3435 Ocean Park BLVD, Suite 203Rajen DhariniAinda não há avaliações
- Case Study LTCSDocumento5 páginasCase Study LTCSKimAinda não há avaliações
- Acid-Base Made EasyDocumento14 páginasAcid-Base Made EasyMayer Rosenberg100% (10)
- Lecture. Physiotherapists. TumoursDocumento34 páginasLecture. Physiotherapists. TumoursdivinaAinda não há avaliações
- Pneumatic RetinopexyDocumento10 páginasPneumatic RetinopexySilpi HamidiyahAinda não há avaliações
- Seminar: DiagnosisDocumento14 páginasSeminar: DiagnosisyenyenAinda não há avaliações
- Medical Nursing RMDocumento11 páginasMedical Nursing RMSharon BaahAinda não há avaliações
- Breast Cancer PresentationDocumento52 páginasBreast Cancer Presentationapi-341607639100% (1)
- Vedic Astrology For Better HealthDocumento27 páginasVedic Astrology For Better HealthJason MintAinda não há avaliações
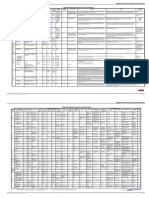
- Case Presentation: Infective EndocarditisDocumento13 páginasCase Presentation: Infective EndocarditisHillaryAinda não há avaliações
- Nursing CS Acute-Kidney-Injury 04Documento1 páginaNursing CS Acute-Kidney-Injury 04Mahdia akterAinda não há avaliações
- Advances in Detection of Fastidious Bacteria - From Microscopic Observation To Molecular BiosensorsDocumento54 páginasAdvances in Detection of Fastidious Bacteria - From Microscopic Observation To Molecular BiosensorsmotohumeresAinda não há avaliações