Você também pode gostar
- Kwong 2012Documento8 páginasKwong 2012Ke XuAinda não há avaliações
- Clinico-Radiological Co-Relation of Carcinoma Larynx and Hypopharynx: A Prospective StudyDocumento7 páginasClinico-Radiological Co-Relation of Carcinoma Larynx and Hypopharynx: A Prospective StudyDede MarizalAinda não há avaliações
- Ijss Jan Oa08Documento7 páginasIjss Jan Oa08IvanDwiKurniawanAinda não há avaliações
- Adeno CaDocumento4 páginasAdeno CaPutri Wulan SukmawatiAinda não há avaliações
- IAEA HPFX 2015Documento6 páginasIAEA HPFX 2015Johana PatiñoAinda não há avaliações
- increasing-neoadjuvant-chemotherapy-in-nasopharyngeal-carcinoma-patientsDocumento4 páginasincreasing-neoadjuvant-chemotherapy-in-nasopharyngeal-carcinoma-patientsMiss AmyAinda não há avaliações
- Neutrophil To Lymphocyte Ratio (NLR) As An Indicator of Poor Prognosis in Stage IV Non-Small Cell Lung CancerDocumento6 páginasNeutrophil To Lymphocyte Ratio (NLR) As An Indicator of Poor Prognosis in Stage IV Non-Small Cell Lung CancerWilliamRayCassidyAinda não há avaliações
- Medi 100 E27450 PDFDocumento6 páginasMedi 100 E27450 PDFVirgiawan WigunaAinda não há avaliações
- Sinonasal Diffuse Large B Cell LymphomaDocumento6 páginasSinonasal Diffuse Large B Cell LymphomaRini RahmawulandariAinda não há avaliações
- Comparison of Clinical and Pathological Features of Lymph Node Tuberculosis and Histiocytic Necrotizing LymphadenitisDocumento8 páginasComparison of Clinical and Pathological Features of Lymph Node Tuberculosis and Histiocytic Necrotizing LymphadenitisfavorendaAinda não há avaliações
- Ca NasopharingDocumento6 páginasCa NasopharingidabagusindrakramasanjayaAinda não há avaliações
- Cancer - 2004 - Li - Treatment Outcome and Pattern of Failure in 77 Patients With Sinonasal Natural Killer T Cell or T CellDocumento10 páginasCancer - 2004 - Li - Treatment Outcome and Pattern of Failure in 77 Patients With Sinonasal Natural Killer T Cell or T Cell2512505993Ainda não há avaliações
- Wagner1994 (No Hace Biopsia)Documento7 páginasWagner1994 (No Hace Biopsia)ouf81Ainda não há avaliações
- Original ArticleDocumento6 páginasOriginal ArticleGaluin KulaimAinda não há avaliações
- annonc_mdw587.026Documento1 páginaannonc_mdw587.026Aaron Paul BernasAinda não há avaliações
- Group 12 Revisi 3Documento7 páginasGroup 12 Revisi 3Nur Apipa DaudAinda não há avaliações
- Necrotizing Pneumonia in Cancer Patients A.8Documento4 páginasNecrotizing Pneumonia in Cancer Patients A.8Manisha UppalAinda não há avaliações
- Adjuvant RadiotherapyDocumento7 páginasAdjuvant Radiotherapyciko momonAinda não há avaliações
- 2021 Metastasis of Clear Cell Renal Cell Carcinoma To The Larynx A Short Literature Review and Presentation of A Rare Case of Prolonged SurvivalDocumento3 páginas2021 Metastasis of Clear Cell Renal Cell Carcinoma To The Larynx A Short Literature Review and Presentation of A Rare Case of Prolonged SurvivalAlfonsoSánchezAinda não há avaliações
- Primaey Neolplasm of The LungDocumento8 páginasPrimaey Neolplasm of The Lungsamuel kefyalewAinda não há avaliações
- Artigo Carcinoma NUTDocumento6 páginasArtigo Carcinoma NUTlorranatayna202201Ainda não há avaliações
- 03 - MACH-NC TumourSite Radio&Onco2011Documento8 páginas03 - MACH-NC TumourSite Radio&Onco2011Omar SettiAinda não há avaliações
- Title: DDGP Versus SMILE in Newly Diagnosed Advanced NaturalDocumento29 páginasTitle: DDGP Versus SMILE in Newly Diagnosed Advanced NaturalAndi Imam Buchari nstAinda não há avaliações
- Lynch Syndrome: Molecular Mechanism and Current Clinical PracticeNo EverandLynch Syndrome: Molecular Mechanism and Current Clinical PracticeNaohiro TomitaAinda não há avaliações
- EORTC Guidelines 2017Documento18 páginasEORTC Guidelines 2017Cata RodriguezAinda não há avaliações
- Efficacy of Intensity-Modulated Radiotherapy With Concurrent Carboplatin in Nasopharyngeal CarcinomaDocumento8 páginasEfficacy of Intensity-Modulated Radiotherapy With Concurrent Carboplatin in Nasopharyngeal CarcinomadenanurbaniazharAinda não há avaliações
- Interstitial Lung Disease After Pleurodesis For Malignant Pleural EffusionDocumento7 páginasInterstitial Lung Disease After Pleurodesis For Malignant Pleural EffusionMomoraAinda não há avaliações
- Bjorl: Surgical Treatment of Severe Laryngomalacia: A Retrospective Study of 11 CasesDocumento5 páginasBjorl: Surgical Treatment of Severe Laryngomalacia: A Retrospective Study of 11 CasesPutri HakimAinda não há avaliações
- SouthAsianJCancer6115-2517942 065939Documento5 páginasSouthAsianJCancer6115-2517942 065939Gibi SupitAinda não há avaliações
- Cutaneous TB in NigerDocumento4 páginasCutaneous TB in NigerRizky ErizkaAinda não há avaliações
- Concurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung CancerDocumento7 páginasConcurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung Cancerdurgesh kumarAinda não há avaliações
- 1 PB 1 PDFDocumento7 páginas1 PB 1 PDFAdel Ciiy OcheAinda não há avaliações
- Leukoplakia or LPR The Misdiagnosis Orf Laryngeal TuberculosisDocumento5 páginasLeukoplakia or LPR The Misdiagnosis Orf Laryngeal Tuberculosisharyo wiryantoAinda não há avaliações
- Treatment Outcomes of Inmates With Pulmonary Tuberculosis in Baquba Penitentiary: A Follow-Up StudyDocumento5 páginasTreatment Outcomes of Inmates With Pulmonary Tuberculosis in Baquba Penitentiary: A Follow-Up StudyTengku Reza MaulanaAinda não há avaliações
- NeurofibromDocumento15 páginasNeurofibromsibel yıldırımAinda não há avaliações
- A Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerDocumento9 páginasA Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerFarizka Dwinda HAinda não há avaliações
- J, Kalita., Et Al. 2016Documento6 páginasJ, Kalita., Et Al. 2016Ubaida AssalwaAinda não há avaliações
- Andreasen 2015Documento6 páginasAndreasen 2015stoia_sebiAinda não há avaliações
- Predictive Value of Nodal Metastases On Local Recurrence in The Management of Differentiated Thyroid Cancer. Retrospective Clinical StudyDocumento6 páginasPredictive Value of Nodal Metastases On Local Recurrence in The Management of Differentiated Thyroid Cancer. Retrospective Clinical StudyuqbaAinda não há avaliações
- Photodynamic Therapy (PDT) For Lung Cancer: The Yorkshire Laser Centre ExperienceDocumento10 páginasPhotodynamic Therapy (PDT) For Lung Cancer: The Yorkshire Laser Centre ExperienceRahmahh FyyAinda não há avaliações
- Incidence of Small Lymph Node Metastases in Patients With Nasopharyngeal Carcinoma: Clinical Implications For Prognosis and TreatmentDocumento7 páginasIncidence of Small Lymph Node Metastases in Patients With Nasopharyngeal Carcinoma: Clinical Implications For Prognosis and TreatmentAdelin Luthfiana FajrinAinda não há avaliações
- Narrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaDocumento6 páginasNarrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaJavier Perez ManriquezAinda não há avaliações
- HN 04-2011 Sublingual Gland Tumors PDFDocumento6 páginasHN 04-2011 Sublingual Gland Tumors PDFHafiz FatmarAinda não há avaliações
- Needle Tract Implantation Following Fine-Needle Aspiration of Thyroid CancerDocumento7 páginasNeedle Tract Implantation Following Fine-Needle Aspiration of Thyroid Cancersalman khanAinda não há avaliações
- 4451 FullDocumento4 páginas4451 FullSukhvinder Singh RanaAinda não há avaliações
- Autoimmune Inner Ear Disease in A Melanoma Patient Treated With PembrolizumabDocumento6 páginasAutoimmune Inner Ear Disease in A Melanoma Patient Treated With PembrolizumabIndRa KaBhuomAinda não há avaliações
- Understanding and Managing Nasopharyngeal CarcinomaDocumento7 páginasUnderstanding and Managing Nasopharyngeal CarcinomaNur Apipa DaudAinda não há avaliações
- Tongue Manuscript - JIMADocumento15 páginasTongue Manuscript - JIMAajay vidyarthiAinda não há avaliações
- PlasmacytomaDocumento3 páginasPlasmacytoma陳彥霖Ainda não há avaliações
- 3781 FullDocumento6 páginas3781 FullSukhvinder Singh RanaAinda não há avaliações
- Yang 2019Documento9 páginasYang 2019Corona FingerAinda não há avaliações
- Incidence of Tuberculosis in Cervical LymphadenopathyDocumento4 páginasIncidence of Tuberculosis in Cervical Lymphadenopathyedy belajar572Ainda não há avaliações
- 565-Article Text-3133-1-10-20220627Documento5 páginas565-Article Text-3133-1-10-20220627elfiahAinda não há avaliações
- Articol TuberculozaDocumento4 páginasArticol TuberculozaLimbi Moderne AplicateAinda não há avaliações
- Review Article: Current Role of Chemotherapy in Nonmetastatic Nasopharyngeal CancerDocumento8 páginasReview Article: Current Role of Chemotherapy in Nonmetastatic Nasopharyngeal Cancerutari wulandari safitriAinda não há avaliações
- Jo2018 3725837Documento7 páginasJo2018 3725837Akansh DattaAinda não há avaliações
- Extranodal Natural Killer T Cell Lymphoma, Nasal.1-1Documento9 páginasExtranodal Natural Killer T Cell Lymphoma, Nasal.1-1kumar biradarAinda não há avaliações
- 3454-Article Text-11501-1-10-20200318Documento4 páginas3454-Article Text-11501-1-10-20200318NuruljannahAinda não há avaliações
- DTH 34 E14981Documento9 páginasDTH 34 E14981Henry WijayaAinda não há avaliações
- Nasopharyngeal Carcinoma in Children and AdolescentsDocumento5 páginasNasopharyngeal Carcinoma in Children and AdolescentsSyifa MunawarahAinda não há avaliações
- "Neurologi" Epilepsi: Kapita SelektaDocumento3 páginas"Neurologi" Epilepsi: Kapita SelektaFegi NugrahaAinda não há avaliações
- 3083 3426 1 SMDocumento6 páginas3083 3426 1 SMAdeLia Nur FitrianaAinda não há avaliações
- Tugas Individu 2 Bahasa InggrisDocumento1 páginaTugas Individu 2 Bahasa InggrisFegi NugrahaAinda não há avaliações
- Maternal and Placental Risk Factors For Developing Necrot 2017 PediatricsDocumento6 páginasMaternal and Placental Risk Factors For Developing Necrot 2017 PediatricsFegi NugrahaAinda não há avaliações
- Forensic Toxicology Analysis of Self-Poisoning Suicidal Deaths in Tehran, Iran Trends Between 2011-2015Documento10 páginasForensic Toxicology Analysis of Self-Poisoning Suicidal Deaths in Tehran, Iran Trends Between 2011-2015Fegi NugrahaAinda não há avaliações
- Bhsa Inggris 1Documento2 páginasBhsa Inggris 1Fegi NugrahaAinda não há avaliações
- The 2011 Medical Molecular Hydrogen Symposium: An Inaugural Symposium of The Journal Medical Gas ResearchDocumento7 páginasThe 2011 Medical Molecular Hydrogen Symposium: An Inaugural Symposium of The Journal Medical Gas ResearchFegi NugrahaAinda não há avaliações
- Forensic Toxicology Analysis of Self-Poisoning Suicidal Deaths in Tehran, Iran Trends Between 2011-2015Documento10 páginasForensic Toxicology Analysis of Self-Poisoning Suicidal Deaths in Tehran, Iran Trends Between 2011-2015Fegi NugrahaAinda não há avaliações
- Medical HypothesesDocumento2 páginasMedical HypothesesFegi NugrahaAinda não há avaliações
- Refarat AnterokoanalDocumento19 páginasRefarat AnterokoanalFegi NugrahaAinda não há avaliações
- Kode ICD 10 THTDocumento6 páginasKode ICD 10 THTFegi Nugraha100% (2)
- Tugas Individu 2 Bahasa InggrisDocumento1 páginaTugas Individu 2 Bahasa InggrisFegi NugrahaAinda não há avaliações
- Longitudinal Follow Up of Chronic Pulmonary Manifestations I - 2017 - Pediatrics PDFDocumento8 páginasLongitudinal Follow Up of Chronic Pulmonary Manifestations I - 2017 - Pediatrics PDFFegi NugrahaAinda não há avaliações
- Bhsa Inggris 1Documento2 páginasBhsa Inggris 1Fegi NugrahaAinda não há avaliações
- FormDocumento4 páginasFormFegi NugrahaAinda não há avaliações
- Akon TigerDocumento3 páginasAkon TigerFegi NugrahaAinda não há avaliações
- What Is Omphalocele?: Jude's StoryDocumento4 páginasWhat Is Omphalocele?: Jude's StoryFegi NugrahaAinda não há avaliações
- Leukocyte Adhesion Deficiency III Report of Two S 2017 Pediatrics NeonatoDocumento2 páginasLeukocyte Adhesion Deficiency III Report of Two S 2017 Pediatrics NeonatoFegi NugrahaAinda não há avaliações
- Pediatric General Surgery DR Bettolli 2014Documento45 páginasPediatric General Surgery DR Bettolli 2014Zlatan ZvizdicAinda não há avaliações
- What Is OmphaloceleDocumento16 páginasWhat Is OmphaloceleFegi NugrahaAinda não há avaliações
- Immunotherapy BrochureDocumento6 páginasImmunotherapy BrochureFegi NugrahaAinda não há avaliações
- Glomerulopati Bengkulu April 2015Documento36 páginasGlomerulopati Bengkulu April 2015Fegi NugrahaAinda não há avaliações
- 5.protein TargettingDocumento11 páginas5.protein TargettingFegi NugrahaAinda não há avaliações
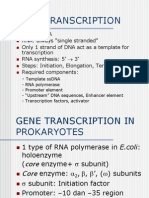
- Gene Transcription 1Documento18 páginasGene Transcription 1Fegi NugrahaAinda não há avaliações
- Pharmaco KineticsDocumento56 páginasPharmaco KineticsFegi NugrahaAinda não há avaliações
- Higher Algebra - Hall & KnightDocumento593 páginasHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Nutrition and CancerDocumento14 páginasNutrition and CancerFegi NugrahaAinda não há avaliações
- Soal B. Inggris Xi - 10Documento6 páginasSoal B. Inggris Xi - 10Fegi NugrahaAinda não há avaliações
- Maintenance Blog by Slackerc0deDocumento15 páginasMaintenance Blog by Slackerc0deFegi NugrahaAinda não há avaliações
- MASM Tutorial PDFDocumento10 páginasMASM Tutorial PDFShashankDwivediAinda não há avaliações
- Ds B2B Data Trans 7027Documento4 páginasDs B2B Data Trans 7027Shipra SriAinda não há avaliações
- 5.1 Physical Farming Constraints in Southern CaliforniaDocumento1 página5.1 Physical Farming Constraints in Southern CaliforniaTom ChiuAinda não há avaliações
- Revised Answer Keys for Scientist/Engineer Recruitment ExamDocumento5 páginasRevised Answer Keys for Scientist/Engineer Recruitment ExamDigantAinda não há avaliações
- Impact of Agile On IT and BusinessDocumento6 páginasImpact of Agile On IT and BusinessPurva RaneAinda não há avaliações
- ENTH 311 Course Video ReflectionDocumento2 páginasENTH 311 Course Video ReflectionJeshua ItemAinda não há avaliações
- Nurses Assigned in Covid-19 Isolation Facilities. in This ConnectionDocumento4 páginasNurses Assigned in Covid-19 Isolation Facilities. in This ConnectionDan HizonAinda não há avaliações
- Affect of CRM-SCM Integration in Retail IndustryDocumento8 páginasAffect of CRM-SCM Integration in Retail IndustryRajeev ChinnappaAinda não há avaliações
- 2015 Masonry Codes and Specifications Compilation, MCAA StoreDocumento1 página2015 Masonry Codes and Specifications Compilation, MCAA StoreMuhammad MurtazaAinda não há avaliações
- Clique Pen's Marketing StrategyDocumento10 páginasClique Pen's Marketing StrategySAMBIT HALDER PGP 2018-20 BatchAinda não há avaliações
- Reviewer in Intermediate Accounting IDocumento9 páginasReviewer in Intermediate Accounting ICzarhiena SantiagoAinda não há avaliações
- Minotaur Transformation by LionWarrior (Script)Documento7 páginasMinotaur Transformation by LionWarrior (Script)Arnt van HeldenAinda não há avaliações
- SOG 5 Topics With SOPDocumento2 páginasSOG 5 Topics With SOPMae Ann VillasAinda não há avaliações
- International Waiver Attestation FormDocumento1 páginaInternational Waiver Attestation FormJiabao ZhengAinda não há avaliações
- Hbet1103 Introduction To General LinguisticsDocumento11 páginasHbet1103 Introduction To General LinguisticsNasidah NasahaAinda não há avaliações
- Essay Sustainable Development GoalsDocumento6 páginasEssay Sustainable Development GoalsBima Dwi Nur Aziz100% (1)
- FeistGorman - 1998-Psychology of Science-Integration of A Nascent Discipline - 2Documento45 páginasFeistGorman - 1998-Psychology of Science-Integration of A Nascent Discipline - 2Josué SalvadorAinda não há avaliações
- Remnan TIIDocumento68 páginasRemnan TIIJOSE MIGUEL SARABIAAinda não há avaliações
- OF Ministry Road Transport Highways (Road Safety Cell) : TH THDocumento3 páginasOF Ministry Road Transport Highways (Road Safety Cell) : TH THAryann Gupta100% (1)
- I Could Easily FallDocumento3 páginasI Could Easily FallBenji100% (1)
- Internet. Social NetworksDocumento22 páginasInternet. Social NetworksjuscatAinda não há avaliações
- The Experience of God Being Consciousness BlissDocumento376 páginasThe Experience of God Being Consciousness BlissVivian Hyppolito100% (6)
- Final Script Tokoh NilamDocumento1 páginaFinal Script Tokoh NilamrayyanAinda não há avaliações
- IAS 8 Tutorial Question (SS)Documento2 páginasIAS 8 Tutorial Question (SS)Given RefilweAinda não há avaliações
- Lecture1 SEODocumento24 páginasLecture1 SEOUsman AnwarAinda não há avaliações
- Fundamentals of Accounting - I FinallDocumento124 páginasFundamentals of Accounting - I Finallyitbarek MAinda não há avaliações
- Global Finance - Introduction ADocumento268 páginasGlobal Finance - Introduction AfirebirdshockwaveAinda não há avaliações
- Relation of Sociology with other social sciencesDocumento4 páginasRelation of Sociology with other social sciencesBheeya BhatiAinda não há avaliações
- 6 Holly Fashion Case StudyDocumento3 páginas6 Holly Fashion Case StudyCaramalau Mirela-Georgiana0% (1)
- Kasapreko PLC Prospectus November 2023Documento189 páginasKasapreko PLC Prospectus November 2023kofiatisu0000Ainda não há avaliações