Você também pode gostar
- Nurul Sakinah Binti Azizan (b041510248)Documento44 páginasNurul Sakinah Binti Azizan (b041510248)sakinah azizanAinda não há avaliações
- Cylinder Design StandardsDocumento8 páginasCylinder Design StandardsterigaliyanAinda não há avaliações
- Medical OxygenDocumento12 páginasMedical Oxygenapi-213031026Ainda não há avaliações
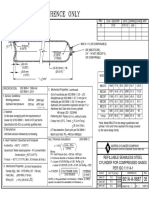
- Refillable Seamless Steel Cylinder For Compressed Gases PER ISO 11114-1Documento1 páginaRefillable Seamless Steel Cylinder For Compressed Gases PER ISO 11114-1bkprodhAinda não há avaliações
- Mitchell Dew Point SensorDocumento2 páginasMitchell Dew Point SensorChris WeirAinda não há avaliações
- Gas Cylinders and GasesDocumento5 páginasGas Cylinders and Gasesjose_mario1128Ainda não há avaliações
- Melaleuca HandbookDocumento54 páginasMelaleuca HandbookDjina StojkovAinda não há avaliações
- Cylinder Retest StationsDocumento8 páginasCylinder Retest StationsjosearrietacoAinda não há avaliações
- SteelDocumento28 páginasSteelAshfaq SaudagarAinda não há avaliações
- Impact of Urbanisation On Water Quality Parameters - A Case Study of Ashtamudi Lake KollamDocumento8 páginasImpact of Urbanisation On Water Quality Parameters - A Case Study of Ashtamudi Lake KollamInternational Journal of Research in Engineering and Technology100% (1)
- Choice of AbutmentDocumento29 páginasChoice of AbutmentSamuel AntobamAinda não há avaliações
- EIGA - Doc 79-19 - Cylinder Retest StationsDocumento11 páginasEIGA - Doc 79-19 - Cylinder Retest StationsDidier GiraldoAinda não há avaliações
- Design and Fabrication of Modern Three Way Dumping Trolley MechanismDocumento8 páginasDesign and Fabrication of Modern Three Way Dumping Trolley MechanismvenkataAinda não há avaliações
- 06 - 60171419 - Centrifugal Pumps - Eng PDFDocumento328 páginas06 - 60171419 - Centrifugal Pumps - Eng PDFRafee Revaldi100% (1)
- Archimedys Technical Data - Metric - GB 11264 PDFDocumento43 páginasArchimedys Technical Data - Metric - GB 11264 PDFAnonymous Cxriyx9HIXAinda não há avaliações
- Deflection LabDocumento9 páginasDeflection LabFarid NajandAinda não há avaliações
- API RP 13C: An Explanation and Answers To Frequently Asked QuestionsDocumento8 páginasAPI RP 13C: An Explanation and Answers To Frequently Asked Questionsmagomago123Ainda não há avaliações
- Seal-Jet Norge As - Sealing SolutionsDocumento73 páginasSeal-Jet Norge As - Sealing SolutionsdanilovoaAinda não há avaliações
- SE SL 9 30 KW DatasheetGB 0412Documento100 páginasSE SL 9 30 KW DatasheetGB 0412GrundfosEgyptAinda não há avaliações
- Brochure - Petrol Station Systems 03 PDFDocumento24 páginasBrochure - Petrol Station Systems 03 PDFTony BombataAinda não há avaliações
- Parts of Oil ExpellerDocumento2 páginasParts of Oil Expellerrahul rkAinda não há avaliações
- Hydraulic CylindersDocumento7 páginasHydraulic Cylinderspacopil34Ainda não há avaliações
- Catalog Rollent 2014 Lite PDFDocumento32 páginasCatalog Rollent 2014 Lite PDFbhq76Ainda não há avaliações
- Belts and RopesDocumento43 páginasBelts and RopesharishankarnadarAinda não há avaliações
- Ongc Report @skandDocumento26 páginasOngc Report @skandSkand JhaAinda não há avaliações
- L13-Rolling of MetalsDocumento32 páginasL13-Rolling of MetalsAbirHasan100% (1)
- Can Crusher ReportDocumento12 páginasCan Crusher ReportHarkirat SinghAinda não há avaliações
- Design of Adjustable Wheel Removal TrolleyDocumento3 páginasDesign of Adjustable Wheel Removal TrolleySelemon AssefaAinda não há avaliações
- Product Design SpecificationDocumento2 páginasProduct Design SpecificationCharlie100% (1)
- Technical Drawings For Toaster Automata 1Documento8 páginasTechnical Drawings For Toaster Automata 1api-371765117Ainda não há avaliações
- Screw PumpsDocumento4 páginasScrew PumpsElia MekdadAinda não há avaliações
- Road Design AspectDocumento30 páginasRoad Design AspectNiken RaharinaAinda não há avaliações
- Lapping ProceduresDocumento3 páginasLapping ProceduresHamza NoumanAinda não há avaliações
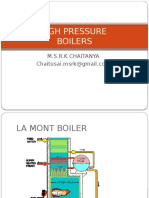
- High Pressure BoilersDocumento15 páginasHigh Pressure BoilersChaitanya MsrkAinda não há avaliações
- Agriculture Reciprocating Sprayer 2222Documento4 páginasAgriculture Reciprocating Sprayer 2222Avneesh BabreAinda não há avaliações
- E04 Using Kalsi Seals in Washpipe AssembliesDocumento17 páginasE04 Using Kalsi Seals in Washpipe AssembliesSuresh Kumar MittapalliAinda não há avaliações
- Angular Depth of Threads CalcDocumento1 páginaAngular Depth of Threads Calcdavidsternleader5768Ainda não há avaliações
- Fittings BookDocumento237 páginasFittings BookFlorina IordanAinda não há avaliações
- Welding Table ProjectDocumento15 páginasWelding Table ProjectKheri MohdAinda não há avaliações
- Velocity and Acceleration Lab Result (Car Ramp)Documento3 páginasVelocity and Acceleration Lab Result (Car Ramp)Ugur ASİT60% (5)
- O RingsDocumento6 páginasO RingsCuepattAinda não há avaliações
- Report Jig and Fixture (Surface Grinding)Documento33 páginasReport Jig and Fixture (Surface Grinding)Shahrul Niezam100% (1)
- ROLLED STEEL BEAMS (Indian Standard) : DesignationDocumento2 páginasROLLED STEEL BEAMS (Indian Standard) : DesignationdramiltAinda não há avaliações
- Braking Systems: By: Rohan Vanjani 1509140125Documento25 páginasBraking Systems: By: Rohan Vanjani 1509140125siddharth johriAinda não há avaliações
- Pnuematic SystemDocumento15 páginasPnuematic SystemAadityaAinda não há avaliações
- S3 Product Range - EnglishDocumento35 páginasS3 Product Range - EnglishJuan Esteban Luque ZegarraAinda não há avaliações
- Layout GuideDocumento9 páginasLayout Guiderapidindustries100% (1)
- Nylon Sleeve CouplingDocumento3 páginasNylon Sleeve CouplingHudiAinda não há avaliações
- BOOK 2, CHAPTER 1 - Hydraulic Accumulators (Part 1) - Other Technologies Content From Hydraulics & PneumaticsDocumento3 páginasBOOK 2, CHAPTER 1 - Hydraulic Accumulators (Part 1) - Other Technologies Content From Hydraulics & PneumaticssourajpatelAinda não há avaliações
- OneSteel Data Charts - FinalDocumento20 páginasOneSteel Data Charts - FinalDaniel CheesmanAinda não há avaliações
- Experiment No: 03 EXPERIMENT: Measurement of Different Parameters of A Machine Component Using The Optical ComparatorDocumento7 páginasExperiment No: 03 EXPERIMENT: Measurement of Different Parameters of A Machine Component Using The Optical ComparatorAbienash Thangavel100% (1)
- Problem Statement For Design For ManufacturingDocumento3 páginasProblem Statement For Design For ManufacturingRob JohnsonAinda não há avaliações
- BASIC HYDRAULICS NDocumento194 páginasBASIC HYDRAULICS NAkshay DandgeAinda não há avaliações
- Melaleuca Compensation PlanDocumento7 páginasMelaleuca Compensation PlanTanka Prasad BhattaraiAinda não há avaliações
- Manual Maquina HidrogenoDocumento35 páginasManual Maquina HidrogenomanuelAinda não há avaliações
- Minor Losses in Bends Lab ReportDocumento8 páginasMinor Losses in Bends Lab Reportalex starrett0% (1)
- Pump VSPDocumento12 páginasPump VSPMiguel V. PalAinda não há avaliações
- Anaesthesia Gas Supply: Gas Cylinders: Review ArticleDocumento7 páginasAnaesthesia Gas Supply: Gas Cylinders: Review ArticleVincent LawAinda não há avaliações
- Anaesthetic Machine Basics 2021Documento20 páginasAnaesthetic Machine Basics 2021Abdullah ZahidAinda não há avaliações
- Prevention of Valve Fugitive Emissions in the Oil and Gas IndustryNo EverandPrevention of Valve Fugitive Emissions in the Oil and Gas IndustryAinda não há avaliações
- Secondary Transport - PactDocumento4 páginasSecondary Transport - PactSanj.etcAinda não há avaliações
- GUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsDocumento83 páginasGUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsSanj.etcAinda não há avaliações
- QBase Anaesthesia 1Documento209 páginasQBase Anaesthesia 1Sanj.etcAinda não há avaliações
- 6 - Glossary - PactDocumento7 páginas6 - Glossary - PactSanj.etcAinda não há avaliações
- Rhabdomyolysis - PACTDocumento2 páginasRhabdomyolysis - PACTSanj.etcAinda não há avaliações
- Transfer of The Critically Ill Patient - PACTDocumento3 páginasTransfer of The Critically Ill Patient - PACTSanj.etcAinda não há avaliações
- Foetal AutopsyDocumento17 páginasFoetal AutopsySanj.etcAinda não há avaliações
- Intravenous FluidsDocumento37 páginasIntravenous FluidsStella UmehAinda não há avaliações
- A Non-Fatal Self-Poisoning Attempt With Sildenafil: by Guest On 11 November 2017Documento5 páginasA Non-Fatal Self-Poisoning Attempt With Sildenafil: by Guest On 11 November 2017Sanj.etcAinda não há avaliações
- 500 SBA Gen Systemic Pathology PDFDocumento27 páginas500 SBA Gen Systemic Pathology PDFSanj.etcAinda não há avaliações
- Med Oncology MCQDocumento109 páginasMed Oncology MCQdrzika100% (8)
- SLCoP Sinhala5405694062132472021Documento1 páginaSLCoP Sinhala5405694062132472021Sanj.etcAinda não há avaliações
- BMI 8 Selection ExamDocumento4 páginasBMI 8 Selection ExamSanj.etcAinda não há avaliações
- Opioid and Non-Opioid Analgesics in The ICUDocumento2 páginasOpioid and Non-Opioid Analgesics in The ICUSanj.etcAinda não há avaliações
- Peripartum Collapse 4.0Documento14 páginasPeripartum Collapse 4.0Sanj.etcAinda não há avaliações
- J Coll Physicians Surg Pak 2014 24 8 603 605Documento3 páginasJ Coll Physicians Surg Pak 2014 24 8 603 605Sanj.etcAinda não há avaliações
- Delirium in Critically IllDocumento37 páginasDelirium in Critically IllSanj.etcAinda não há avaliações
- 128 Diabetic KetoacidosisDocumento9 páginas128 Diabetic KetoacidosisDite Bayu NugrohoAinda não há avaliações
- Management of Safe AnaesthesiaDocumento38 páginasManagement of Safe AnaesthesiaSanj.etcAinda não há avaliações
- Antimicrobial Stewardship Systems and Processes For Effective Antimicrobial Medicine Use PDF 1837273110469Documento52 páginasAntimicrobial Stewardship Systems and Processes For Effective Antimicrobial Medicine Use PDF 1837273110469Sanj.etcAinda não há avaliações
- Endgames: Acute EpiglottitisDocumento3 páginasEndgames: Acute EpiglottitisSanj.etcAinda não há avaliações
- Epidurals and Spinals - Apr16Documento6 páginasEpidurals and Spinals - Apr16Sanj.etcAinda não há avaliações
- Ain ShamsJAnaesthesiol73336 7108132 - 015828Documento4 páginasAin ShamsJAnaesthesiol73336 7108132 - 015828Sanj.etcAinda não há avaliações
- SSCBundleCard PrintDocumento2 páginasSSCBundleCard PrintSanj.etcAinda não há avaliações
- Emergency Laparotomy: Patient Information FactsheetDocumento4 páginasEmergency Laparotomy: Patient Information FactsheetMuhammad RizqiAinda não há avaliações
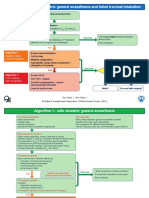
- 01 15 DAS Algorithms Web PRINT20092015Documento6 páginas01 15 DAS Algorithms Web PRINT20092015Sanj.etcAinda não há avaliações
- Saline IV Fluid ComparisonDocumento2 páginasSaline IV Fluid ComparisonSanj.etcAinda não há avaliações
- Anaesthesia For Major Abdominal SurgeryDocumento1 páginaAnaesthesia For Major Abdominal SurgerySanj.etcAinda não há avaliações
- IV Fluid ChartDocumento2 páginasIV Fluid Charthady920Ainda não há avaliações
- MS DirectPhD Sample PDFDocumento4 páginasMS DirectPhD Sample PDFArunKumarAinda não há avaliações
- Recycling of Li Ion Batteries EUDocumento28 páginasRecycling of Li Ion Batteries EUdcahyasturaAinda não há avaliações
- Biodegradation of Keratin Waste Theory and Practical AspectsDocumento13 páginasBiodegradation of Keratin Waste Theory and Practical AspectsRodrigo Lara100% (1)
- Khairat Al-Emar Co. For Oil Services: Material Safety Data SheetDocumento6 páginasKhairat Al-Emar Co. For Oil Services: Material Safety Data SheetqwaszxcdeAinda não há avaliações
- United States Patent: (45) Date of Patent: Aug - 21, 2018Documento22 páginasUnited States Patent: (45) Date of Patent: Aug - 21, 2018RiskaAinda não há avaliações
- Indra: For ConstructionDocumento25 páginasIndra: For Constructionsumit kumarAinda não há avaliações
- Sika PDS E Intraplast ZDocumento2 páginasSika PDS E Intraplast Zlwin_oo2435100% (1)
- Recrystallization: Activity No. 6Documento6 páginasRecrystallization: Activity No. 6Mary Jean SteffenAinda não há avaliações
- 110 WS Gas Stoichiometry KeyDocumento2 páginas110 WS Gas Stoichiometry Keyエルミタ ジョイ ファティマ100% (1)
- Risk Management PlanDocumento2 páginasRisk Management PlanRoxanneGailBigcasGoleroAinda não há avaliações
- In Silico Sequence Analysis, Homology Modeling and Function Annotation of Ocimum Basilicum Hypothetical Protein G1CT28 - OCIBADocumento8 páginasIn Silico Sequence Analysis, Homology Modeling and Function Annotation of Ocimum Basilicum Hypothetical Protein G1CT28 - OCIBAmariohuangAinda não há avaliações
- Mock Test 04 LCDocumento9 páginasMock Test 04 LCielts Ice GiangAinda não há avaliações
- IPPP II (Cosmetics)Documento46 páginasIPPP II (Cosmetics)Tinsaye HayileAinda não há avaliações
- Vanadium and Vanadium CompoundsDocumento21 páginasVanadium and Vanadium CompoundsПлейнAinda não há avaliações
- Boq 153501Documento28 páginasBoq 153501kamakhyaguri pwdAinda não há avaliações
- Castrol The Oil FactorDocumento19 páginasCastrol The Oil FactorPrabhu LohakareAinda não há avaliações
- The BTX Chain: Benzene, Toluene, XyleneDocumento36 páginasThe BTX Chain: Benzene, Toluene, XyleneSorina CernatAinda não há avaliações
- Recommended Construction Guidelines For Full Depth Reclamation (FDR) Using Bituminous StabilizationDocumento13 páginasRecommended Construction Guidelines For Full Depth Reclamation (FDR) Using Bituminous StabilizationDao Phuc LamAinda não há avaliações
- Chlorine Dioxide: Chlorophenol Red Method Method 8065 0.01 To 1.00 MG/L Clo (LR)Documento6 páginasChlorine Dioxide: Chlorophenol Red Method Method 8065 0.01 To 1.00 MG/L Clo (LR)Oudah AliAinda não há avaliações
- Chemical Ecology of VertebratesDocumento578 páginasChemical Ecology of VertebratesJulio MoraesAinda não há avaliações
- Analisis Fitokimia Daun Pepaya (Carica Papaya L.) A'yun Et Al.Documento7 páginasAnalisis Fitokimia Daun Pepaya (Carica Papaya L.) A'yun Et Al.Cahaya Medika1Ainda não há avaliações
- AnchorDocumento5 páginasAnchorpadalakirankumarAinda não há avaliações
- Functionalization of GrapheneDocumento59 páginasFunctionalization of GrapheneDiego Alejandro Hurtado BalcazarAinda não há avaliações
- Speedy Moisture AASHTO T217Documento3 páginasSpeedy Moisture AASHTO T217dep_vinAinda não há avaliações
- Faizal Bux, Yusuf Chisti Eds. Algae Biotechnology Products and ProcessesDocumento344 páginasFaizal Bux, Yusuf Chisti Eds. Algae Biotechnology Products and ProcessesHAMED100% (4)
- Isi BukuDocumento183 páginasIsi BukuHayat Hamzah DawiAinda não há avaliações
- Drying in Mass TransferDocumento57 páginasDrying in Mass TransferMohammad JunaidAinda não há avaliações
- Prria MemoDocumento4 páginasPrria MemoRebecca C. LewisAinda não há avaliações
- Catalogue DM AhuDocumento54 páginasCatalogue DM AhurianaAinda não há avaliações