Você também pode gostar
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionNo EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionAinda não há avaliações
- Intraoperative NotesDocumento22 páginasIntraoperative NotesIsabel AranconAinda não há avaliações
- Operating Room Orientation Manual Goals &Documento4 páginasOperating Room Orientation Manual Goals &bhuselleAinda não há avaliações
- Scrub Nurse1Documento50 páginasScrub Nurse1Amy Lalringhluani Chhakchhuak100% (1)
- GENERAL SAFETY CHECKLIST GuidelinesDocumento10 páginasGENERAL SAFETY CHECKLIST GuidelinesTina AlteranAinda não há avaliações
- Operating Room Personnel OrganizationDocumento4 páginasOperating Room Personnel OrganizationantihistamiiineAinda não há avaliações
- Circulating NurseDocumento3 páginasCirculating NurseSoheil LimboAinda não há avaliações
- Intra Op CombinedDocumento62 páginasIntra Op CombinedJan Federick Bantay100% (1)
- 16/12/12 Army Force Comphensive Specialized Hospital or Department Standard /sop/ Nursing DutiesDocumento7 páginas16/12/12 Army Force Comphensive Specialized Hospital or Department Standard /sop/ Nursing DutiesSuzy BaeAinda não há avaliações
- Perioperative Nursing Care for PatientsDocumento50 páginasPerioperative Nursing Care for PatientsPreeti ChouhanAinda não há avaliações
- Pre-Operative Nursing CareDocumento79 páginasPre-Operative Nursing CarePeter FrimpongAinda não há avaliações
- IntraoperativeDocumento4 páginasIntraoperativeLynette Roldan RN100% (1)
- Principles of Sterile TechniqueDocumento3 páginasPrinciples of Sterile TechniqueMaria VisitacionAinda não há avaliações
- OR Duty RLE RequirementsDocumento5 páginasOR Duty RLE RequirementsSammy Jr FamilarAinda não há avaliações
- SURGICAL INSTRUMENTS GUIDEDocumento137 páginasSURGICAL INSTRUMENTS GUIDEMelchor Felipe Salvosa100% (1)
- Surgical Hand Scrub Protocol UpdatesDocumento22 páginasSurgical Hand Scrub Protocol UpdatesRex Lagunzad Flores100% (2)
- Assisted Gowning & GlovingDocumento12 páginasAssisted Gowning & GlovingCarmina GurreaAinda não há avaliações
- Bandage and Sling Guide for Wound CareDocumento47 páginasBandage and Sling Guide for Wound Careriza sarmientoAinda não há avaliações
- Or Rle 1-1Documento23 páginasOr Rle 1-1Jan Federick Bantay100% (1)
- Etiquette and PrinciplesDocumento3 páginasEtiquette and PrinciplesHoney Bee S. PlatolonAinda não há avaliações
- Scrubbing Gowning and Gloving LECTUREDocumento5 páginasScrubbing Gowning and Gloving LECTUREEyji GeronimoAinda não há avaliações
- What Is Aseptic TechniqueDocumento11 páginasWhat Is Aseptic TechniqueMarlchiel Nathan ArregladoAinda não há avaliações
- Donning of Personal Protective Equipment (PPE) Procedure ChecklistDocumento3 páginasDonning of Personal Protective Equipment (PPE) Procedure ChecklistMonicaElizadePazAinda não há avaliações
- Insulin Injection Technique GuideDocumento23 páginasInsulin Injection Technique Guideimamori100% (1)
- Post Operative MGTDocumento10 páginasPost Operative MGTNatukunda DianahAinda não há avaliações
- I. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordDocumento2 páginasI. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordERWINAinda não há avaliações
- 20 Common Surgical Instruments in ErDocumento8 páginas20 Common Surgical Instruments in ErMelissa GoAinda não há avaliações
- Scrub Nurse Circulating NurseDocumento2 páginasScrub Nurse Circulating NurseLalaine Nadulpit100% (2)
- TAHBSO Procedure ExplainedDocumento14 páginasTAHBSO Procedure ExplainedDafny CzarinaAinda não há avaliações
- Operating Room TeamDocumento7 páginasOperating Room TeamFaruqueHossain100% (1)
- Operating Room TechniqueDocumento5 páginasOperating Room TechniquerootieAinda não há avaliações
- Or AssignmentDocumento5 páginasOr AssignmentJohara MacasindelAinda não há avaliações
- START Triage Training PresentationDocumento85 páginasSTART Triage Training PresentationPandu Putra Wijaya RestaAinda não há avaliações
- Patient Positioning in Operating TheatreDocumento52 páginasPatient Positioning in Operating TheatreFatkhul AdhiatmadjaAinda não há avaliações
- CsDocumento7 páginasCsakosiMJcutie100% (1)
- Perioperative NSG Care MGTDocumento56 páginasPerioperative NSG Care MGTinchack100% (1)
- Operating Room ProcedureDocumento4 páginasOperating Room ProcedureROxanne S. RendonAinda não há avaliações
- Surgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingDocumento55 páginasSurgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingCathreen Agatha Fule100% (1)
- COMMON ORTHOPEDIC INSTRUMENTSDocumento16 páginasCOMMON ORTHOPEDIC INSTRUMENTSCosmic PhilippinesAinda não há avaliações
- Or ExamDocumento21 páginasOr Examlouie roderosAinda não há avaliações
- Fracture (Cast Care)Documento6 páginasFracture (Cast Care)Vane UcatAinda não há avaliações
- Preoperative Checklist-1Documento10 páginasPreoperative Checklist-1June Faith HacheroAinda não há avaliações
- Critical Care NursingDocumento2 páginasCritical Care NursingJyoti KathAinda não há avaliações
- Pre Op ChecklistDocumento1 páginaPre Op ChecklistKoushik Reddy PodduturiAinda não há avaliações
- Perioperative NursingDocumento155 páginasPerioperative NursingEissac100% (1)
- Operating Room Nursing: S Y 2018-2019 FIRST SEMDocumento29 páginasOperating Room Nursing: S Y 2018-2019 FIRST SEMMaria Sheila BelzaAinda não há avaliações
- Perioperative NursingDocumento74 páginasPerioperative NursingTina Talmadge100% (4)
- Thyroidectomy GuideDocumento19 páginasThyroidectomy GuideKatrina Ponce100% (4)
- Surgical ScrubbingDocumento2 páginasSurgical ScrubbingAnn Mayie100% (1)
- Skin PreparationDocumento2 páginasSkin Preparationoxidalaj100% (24)
- Colostomy Irrigation ProcedureDocumento24 páginasColostomy Irrigation ProcedureJan Federick Bantay100% (1)
- Who Safe Surgery Checklist: Sign inDocumento3 páginasWho Safe Surgery Checklist: Sign inJann Marie IsidroAinda não há avaliações
- ID-IM-SQ-E ToolDocumento9 páginasID-IM-SQ-E TooltriciacamilleAinda não há avaliações
- 13 Aseptic TechniqueDocumento6 páginas13 Aseptic TechniqueaironmaeAinda não há avaliações
- Simple Triage and Rapid TreatmentDocumento9 páginasSimple Triage and Rapid TreatmentGung IndrayanaAinda não há avaliações
- Principles of Patient PositioningDocumento62 páginasPrinciples of Patient PositioningMelody JusticeAinda não há avaliações
- Duties of Circulating NurseDocumento11 páginasDuties of Circulating NurseHuemer Uy100% (1)
- Duties and Responsibilities of Nurses in OtDocumento5 páginasDuties and Responsibilities of Nurses in Otvinnu kalyan100% (1)
- Dutiesof Scrub and Circulating NurseDocumento1 páginaDutiesof Scrub and Circulating NursedammenoelAinda não há avaliações
- Duties of scrub and circulating nurses (38Documento12 páginasDuties of scrub and circulating nurses (38ckimkimkimAinda não há avaliações
- Renal CalculiDocumento28 páginasRenal Calculihailleyann33% (3)
- NCP CalculiDocumento8 páginasNCP CalculihailleyannAinda não há avaliações
- Eclampsia OutputDocumento5 páginasEclampsia OutputhailleyannAinda não há avaliações
- Placenta PraeviaDocumento10 páginasPlacenta PraeviahailleyannAinda não há avaliações
- CP FinalDocumento53 páginasCP FinalhailleyannAinda não há avaliações
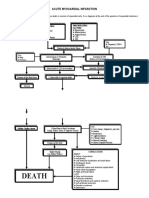
- Acute Myocardial InfarctionDocumento2 páginasAcute Myocardial InfarctionhailleyannAinda não há avaliações
- PaThoPhysiology of EclampsiaDocumento5 páginasPaThoPhysiology of Eclampsiahailleyann100% (2)
- Sysman Safety-Integrated-5ed en PDFDocumento345 páginasSysman Safety-Integrated-5ed en PDFErdincAinda não há avaliações
- Informed Consent and Release, Waiver, and Quitclaim: Know All Men by These PresentsDocumento2 páginasInformed Consent and Release, Waiver, and Quitclaim: Know All Men by These PresentsRobee Camille Desabelle-SumatraAinda não há avaliações
- NUST Hostel Admission Form New PDFDocumento2 páginasNUST Hostel Admission Form New PDFMuhammad Waqas0% (1)
- The Costly Business of DiscriminationDocumento46 páginasThe Costly Business of DiscriminationCenter for American Progress100% (1)
- Journal On The Impact of Nursing Informatics To Clinical PracticeDocumento2 páginasJournal On The Impact of Nursing Informatics To Clinical PracticeLhara Vhaneza CuetoAinda não há avaliações
- OPD Network ListDocumento354 páginasOPD Network ListSHAIKH ABDUL AZIZ salim bashaAinda não há avaliações
- TIVA Part I - Pharmacokinetic Principles and Methods of Delivery PDFDocumento56 páginasTIVA Part I - Pharmacokinetic Principles and Methods of Delivery PDFMaria José RecheAinda não há avaliações
- hdf492 Portfolio PresentationDocumento14 páginashdf492 Portfolio Presentationapi-403412647Ainda não há avaliações
- Central Adult and Pediatric in Tensive Care UnitDocumento4 páginasCentral Adult and Pediatric in Tensive Care UnitChris T NaAinda não há avaliações
- Stericon Plus BioindicatorDocumento4 páginasStericon Plus Bioindicatorupt labkeswanbaliAinda não há avaliações
- Methodological Literature Review 1 1Documento8 páginasMethodological Literature Review 1 1api-584018105Ainda não há avaliações
- Epilepsy and LevetiracetamDocumento53 páginasEpilepsy and LevetiracetamHasan Ahmed KhanAinda não há avaliações
- RNTCP - Wikipedia, The Free EncyclopediaDocumento5 páginasRNTCP - Wikipedia, The Free EncyclopediaakurilAinda não há avaliações
- Yoga Your Home Practice CompanionDocumento257 páginasYoga Your Home Practice Companionjohncoltrane97% (33)
- Immunology Serology Blood BankingDocumento5 páginasImmunology Serology Blood BankingEdsss Villar100% (3)
- Table : Number of Population, Hospitals and Beds in All Over JordanDocumento8 páginasTable : Number of Population, Hospitals and Beds in All Over JordanjAinda não há avaliações
- Intro To Wastewater Collection and PumpingDocumento84 páginasIntro To Wastewater Collection and PumpingMoh'd KhadAinda não há avaliações
- Effectiveness of exercise therapy and infrared therapy for shoulder dislocationDocumento11 páginasEffectiveness of exercise therapy and infrared therapy for shoulder dislocationhobi kitaAinda não há avaliações
- Safety Reports Series No. 13 (Radiation Protection and Safety in Industrial Radiography)Documento69 páginasSafety Reports Series No. 13 (Radiation Protection and Safety in Industrial Radiography)jalsadidiAinda não há avaliações
- Adult Health - Soap Note 5Documento3 páginasAdult Health - Soap Note 5api-546259691100% (3)
- UV-VIS Method for Estimating Fat-Soluble Vitamins in MultivitaminsDocumento6 páginasUV-VIS Method for Estimating Fat-Soluble Vitamins in MultivitaminsTisenda TimiselaAinda não há avaliações
- Complaints Handling: BDA AdviceDocumento8 páginasComplaints Handling: BDA Advicedruzair007Ainda não há avaliações
- Oferta Hexis - Multisign: Preturile Sunt in EURO Si Nu Includ TVADocumento9 páginasOferta Hexis - Multisign: Preturile Sunt in EURO Si Nu Includ TVAPoschina CiprianAinda não há avaliações
- Domestic Physician HeringDocumento490 páginasDomestic Physician Heringskyclad_21Ainda não há avaliações
- Eo No. 013 - 2018 Reorganization of BhertDocumento2 páginasEo No. 013 - 2018 Reorganization of BhertAnne Kimberly Peñalba BabaanAinda não há avaliações
- Research Paper About EpilepsyDocumento4 páginasResearch Paper About EpilepsyHazel Anne Joyce Antonio100% (1)
- Technology and Livelihood Education: Quarter 1 - Module 4: CaregivingDocumento20 páginasTechnology and Livelihood Education: Quarter 1 - Module 4: CaregivingIrine Irine100% (1)
- Birth Injuries: Causes, Types and TreatmentDocumento9 páginasBirth Injuries: Causes, Types and TreatmentshailaAinda não há avaliações
- 2012 Bringing Our Dying HomeDocumento68 páginas2012 Bringing Our Dying HomeendofliferesearchAinda não há avaliações