Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Pharm I - Abx ChartDocumento4 páginasPharm I - Abx ChartNicole BerryAinda não há avaliações
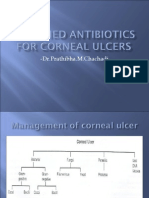
- Fortified AntibioticsDocumento25 páginasFortified Antibioticsch_prathi7654100% (9)
- MKSAP 16 - Infectious DiseaseDocumento340 páginasMKSAP 16 - Infectious DiseaseBacanator75% (4)
- Pharm Practice QuestionsDocumento42 páginasPharm Practice QuestionsShannon Garcia100% (1)
- VancomycinDocumento1 páginaVancomycinE100% (2)
- Introduction To PharmacologyDocumento119 páginasIntroduction To PharmacologyYzel Vasquez AdavanAinda não há avaliações
- SepticemiaDocumento171 páginasSepticemiaThashini Devi Nagaratnam100% (1)
- The Use of Vancomycin With Its Therapeutic and Adverse Effects: A ReviewDocumento11 páginasThe Use of Vancomycin With Its Therapeutic and Adverse Effects: A Reviewdea yuniarAinda não há avaliações
- JPN 321 Autumn 2019 PDFDocumento60 páginasJPN 321 Autumn 2019 PDFjumantoAinda não há avaliações
- Vancomycin Dosing and Monitoring in AdultsDocumento1 páginaVancomycin Dosing and Monitoring in AdultsjulialeoAinda não há avaliações
- Antib 2020 - LB Engl Prima Varianta Fara CorecturiDocumento13 páginasAntib 2020 - LB Engl Prima Varianta Fara CorecturiIrina Panciu StefanAinda não há avaliações
- Antibiotic Desensitization ProtocolsDocumento7 páginasAntibiotic Desensitization ProtocolsMichael FreudigerAinda não há avaliações
- OPAT Anti-Infective Administration MethodsDocumento6 páginasOPAT Anti-Infective Administration MethodsNikki TranAinda não há avaliações
- Antibiotic Resistance in Wastewater BacteriaDocumento14 páginasAntibiotic Resistance in Wastewater BacteriaraowaleedahmadAinda não há avaliações
- Drug StudyDocumento3 páginasDrug StudyFloribelle SamaniegoAinda não há avaliações
- Presentation SSIDocumento41 páginasPresentation SSIJawad Mustafa100% (1)
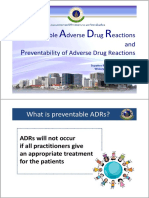
- P A D R: Reventable Dverse Rug Eactions and Reventability of Adverse Drug ReactionsDocumento22 páginasP A D R: Reventable Dverse Rug Eactions and Reventability of Adverse Drug Reactionsarisara duemkhanAinda não há avaliações
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocumento11 páginasSummary of Product Characteristics: 4.1 Therapeutic IndicationsAninditaSahaAinda não há avaliações
- Vancomycin TDMDocumento24 páginasVancomycin TDMAbubakr AurangzebAinda não há avaliações
- Developed by Joenny - King at Ebay - Com (Will NotDocumento8.250 páginasDeveloped by Joenny - King at Ebay - Com (Will NottcabanilAinda não há avaliações
- EU STIMULAN Digital Brochure MA0074R6Documento20 páginasEU STIMULAN Digital Brochure MA0074R6Nitin JunejaAinda não há avaliações
- Review Questions On Antiviral and AntibioticDocumento63 páginasReview Questions On Antiviral and AntibioticusedforfunplocAinda não há avaliações
- Patients With Multiple DisordersDocumento7 páginasPatients With Multiple DisordersKathleen Joy PingenAinda não há avaliações
- Clinical and Microbiological Effect of Linezolid On Methicillin-ResistantDocumento10 páginasClinical and Microbiological Effect of Linezolid On Methicillin-ResistantNoha GamalAinda não há avaliações
- Antimicrobial Prescribing Delafloxacin For Acute Bacterial Skin and Skin Structure Infections PDF 1158232915141Documento6 páginasAntimicrobial Prescribing Delafloxacin For Acute Bacterial Skin and Skin Structure Infections PDF 1158232915141carlettino7Ainda não há avaliações
- Practice Final Exam2Documento6 páginasPractice Final Exam2johnsonnbrandieAinda não há avaliações
- PNLE Comprehensive 4Documento18 páginasPNLE Comprehensive 4Mon De VeraAinda não há avaliações
- Multiple Drug ResistanceDocumento14 páginasMultiple Drug ResistanceHarsh ChopraAinda não há avaliações
- Clinical Practice Guidelines For Antimicrobial Prophylaxis in Surgery (Update 2013)Documento89 páginasClinical Practice Guidelines For Antimicrobial Prophylaxis in Surgery (Update 2013)เด็กชายสมันตภัทร แฟนคลับอาจารย์กวงAinda não há avaliações
- Pharmacology II OutlineDocumento52 páginasPharmacology II Outlinerjones53Ainda não há avaliações