Você também pode gostar
- Tugas Kgds Analisis Kasus IiDocumento6 páginasTugas Kgds Analisis Kasus Iisepta dwi anggrainiAinda não há avaliações
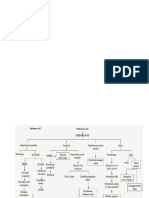
- Patway SCDocumento3 páginasPatway SCsepta dwi anggrainiAinda não há avaliações
- Tugas Kgds Analisis Kasus IiDocumento6 páginasTugas Kgds Analisis Kasus Iisepta dwi anggrainiAinda não há avaliações
- Patway AkiDocumento1 páginaPatway Akisepta dwi anggrainiAinda não há avaliações
- Patway SCDocumento3 páginasPatway SCsepta dwi anggrainiAinda não há avaliações
- Patway AkiDocumento1 páginaPatway Akisepta dwi anggrainiAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Selectable Markers For Animal Cells: Thymidine Kinase (TK), Dihydrofolate Reductase (DHFR), Chloramphenicol Acetyl Transferase (CAT)Documento10 páginasSelectable Markers For Animal Cells: Thymidine Kinase (TK), Dihydrofolate Reductase (DHFR), Chloramphenicol Acetyl Transferase (CAT)MadhwiAinda não há avaliações
- Juvenileidiopathic Arthritis: Peter J. Gowdie,, Shirley M.L. TseDocumento27 páginasJuvenileidiopathic Arthritis: Peter J. Gowdie,, Shirley M.L. TseFandi ArgiansyaAinda não há avaliações
- EORTC Guidelines 2017Documento18 páginasEORTC Guidelines 2017Cata RodriguezAinda não há avaliações
- Anticancer DrugDocumento29 páginasAnticancer DrugAnjana PaudelAinda não há avaliações
- 170 FullDocumento4 páginas170 FullRegita LatuihamalloAinda não há avaliações
- Serbian Association of Dermatovenereologists Guidelines For The Diagnosis and Treatment of PsoriasisDocumento18 páginasSerbian Association of Dermatovenereologists Guidelines For The Diagnosis and Treatment of PsoriasisAndjela KosticAinda não há avaliações
- Conchem q4 Module 4Documento10 páginasConchem q4 Module 4Tiffany Moore100% (1)
- Sce Rheum at Ology Sample QDocumento42 páginasSce Rheum at Ology Sample QZoya AnnamAinda não há avaliações
- A. Antineoplastic DrugsDocumento48 páginasA. Antineoplastic DrugsKim Shyen BontuyanAinda não há avaliações
- Understanding Musculoskeletal DisordersDocumento66 páginasUnderstanding Musculoskeletal DisordersYolla LitaAinda não há avaliações
- Hepatotoxicity During Maintenance Therapy and PrognosisDocumento6 páginasHepatotoxicity During Maintenance Therapy and PrognosisRonnyMulyonoAinda não há avaliações
- Dexamethasone and Methotrexate Drug StudyDocumento4 páginasDexamethasone and Methotrexate Drug StudyJunel Paolo SilvioAinda não há avaliações
- Journal Reading Survey OphtalmologyDocumento17 páginasJournal Reading Survey OphtalmologynadyajondriAinda não há avaliações
- Formilleza, Juripae - Drug Study and NCPDocumento8 páginasFormilleza, Juripae - Drug Study and NCPPatricia FormillezaAinda não há avaliações
- 1Documento10 páginas1drnsatyaprasadAinda não há avaliações
- Juvenile Idiopathic ArthritisDocumento6 páginasJuvenile Idiopathic ArthritissitharAinda não há avaliações
- Subba RaoDocumento5 páginasSubba Raosingh1910511753100% (1)
- Ketoprofen PMDocumento39 páginasKetoprofen PMWahyu AttariaAinda não há avaliações
- Antineoplastics AgentsDocumento19 páginasAntineoplastics AgentsPrincess Diannejane MurlaAinda não há avaliações
- Grade9 STE Con.-Chem. Q4 Module-4 Wk5 ADMDocumento20 páginasGrade9 STE Con.-Chem. Q4 Module-4 Wk5 ADMChelzy CatabasAinda não há avaliações
- Choriocarcinoma 11Documento23 páginasChoriocarcinoma 11Fakhir HasanAinda não há avaliações
- Anticancer DrugsDocumento117 páginasAnticancer DrugsKishore Chandra Korada100% (2)
- Psoriasis Which Therapy For Which PatientDocumento11 páginasPsoriasis Which Therapy For Which PatientWenny AgustinAinda não há avaliações
- Asparaginase / Erwinia AsparaginaseDocumento10 páginasAsparaginase / Erwinia AsparaginaseMohammed HaiderAinda não há avaliações
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocumento9 páginasDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoAinda não há avaliações
- MS Drug StudyDocumento16 páginasMS Drug StudyNathaniel VelascoAinda não há avaliações
- 0002 Rheumatology Notes 2015.... 49Documento58 páginas0002 Rheumatology Notes 2015.... 49Abdul QuyyumAinda não há avaliações
- Anti - Neoplastic & ChemotherapyDocumento63 páginasAnti - Neoplastic & ChemotherapyLisa JessicaAinda não há avaliações
- Metotreksat I FajzerDocumento11 páginasMetotreksat I FajzergregorimAinda não há avaliações