Você também pode gostar
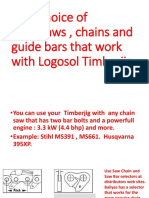
- Your Choice of Chainsaws, Chains and Guide Bars That Work With Logosol TimberjigDocumento6 páginasYour Choice of Chainsaws, Chains and Guide Bars That Work With Logosol TimberjigDiego A Echavarría AAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Overview of The ANSI/HFES 100 - 2007 Ergonomic Standard: A New Standard Is ReleasedDocumento1 páginaOverview of The ANSI/HFES 100 - 2007 Ergonomic Standard: A New Standard Is ReleasedDiego A Echavarría AAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Task AnalisisDocumento43 páginasTask AnalisisDiego A Echavarría AAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- 2022 State of Medical Device ReportDocumento38 páginas2022 State of Medical Device ReportDiego A Echavarría AAinda não há avaliações
- MHAC-An Assessment Tool For Analysing Manual Material Handling TasksDocumento14 páginasMHAC-An Assessment Tool For Analysing Manual Material Handling TasksDiego A Echavarría AAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Assessment of The Ergonomic Risk From Saddle and CDocumento14 páginasAssessment of The Ergonomic Risk From Saddle and CDiego A Echavarría AAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Workplace Ergonomic Guide Darcor Final January 2015Documento14 páginasWorkplace Ergonomic Guide Darcor Final January 2015Diego A Echavarría AAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Human Centric Lighting: Ir. Jasmien Vander Beken January 2019Documento13 páginasHuman Centric Lighting: Ir. Jasmien Vander Beken January 2019Diego A Echavarría AAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Validity and Reliability of A Dental Operator Posture Assessment Instrument (PAI)Documento10 páginasValidity and Reliability of A Dental Operator Posture Assessment Instrument (PAI)Diego A Echavarría AAinda não há avaliações
- Quality Assessment of The University Classroom Lighting - A Case StudyDocumento8 páginasQuality Assessment of The University Classroom Lighting - A Case StudyDiego A Echavarría AAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Visual Ergonomics in The Workplace: Vision and LightingDocumento11 páginasVisual Ergonomics in The Workplace: Vision and LightingDiego A Echavarría AAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Design Principles For Green Ergonomics: April 2013Documento6 páginasDesign Principles For Green Ergonomics: April 2013Diego A Echavarría AAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- A Literature Review of The Effects of Natural Light On Building OccupantsDocumento58 páginasA Literature Review of The Effects of Natural Light On Building OccupantsDiego A Echavarría AAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Benefits of Natural Light: January-February 2014Documento3 páginasThe Benefits of Natural Light: January-February 2014Diego A Echavarría AAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Daylight For Health and Efficiency - A New Career For An Old FriendDocumento8 páginasDaylight For Health and Efficiency - A New Career For An Old FriendDiego A Echavarría AAinda não há avaliações
- Visual Ergonomics: Solutions For Lighting & Eye Health: Tel: 604-822-9040 Fax: 604-822-0572 Ergonomics - Info@ubc - CaDocumento7 páginasVisual Ergonomics: Solutions For Lighting & Eye Health: Tel: 604-822-9040 Fax: 604-822-0572 Ergonomics - Info@ubc - CaDiego A Echavarría AAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Effects of Exposure To Natural Light in The.5Documento19 páginasThe Effects of Exposure To Natural Light in The.5Diego A Echavarría AAinda não há avaliações
- b531 PDFDocumento14 páginasb531 PDFDiego A Echavarría AAinda não há avaliações
- Task Lighting Solutions: Their Economic and Ergonomic BenefitsDocumento8 páginasTask Lighting Solutions: Their Economic and Ergonomic BenefitsDiego A Echavarría AAinda não há avaliações
- Visual Ergonomics in The Workplace: Continuing EducationDocumento7 páginasVisual Ergonomics in The Workplace: Continuing EducationDiego A Echavarría AAinda não há avaliações
- Dhs - Oha: Office Light Management GuideDocumento17 páginasDhs - Oha: Office Light Management GuideDiego A Echavarría AAinda não há avaliações
- Lighting Design in Workplaces: A Case Study of A Modern Library Building in Sheffield, UKDocumento8 páginasLighting Design in Workplaces: A Case Study of A Modern Library Building in Sheffield, UKDiego A Echavarría AAinda não há avaliações
- Optometry: From Visual Performance To Visual Ergonomics: A Personal Historic ViewDocumento7 páginasOptometry: From Visual Performance To Visual Ergonomics: A Personal Historic ViewDiego A Echavarría AAinda não há avaliações
- Daylight and The Workplace Study: Your Window To WellnessDocumento12 páginasDaylight and The Workplace Study: Your Window To WellnessDiego A Echavarría AAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hung Et Al-2009-Human Factors and Ergonomics in Manufacturing & Service Industries PDFDocumento16 páginasHung Et Al-2009-Human Factors and Ergonomics in Manufacturing & Service Industries PDFDiego A Echavarría AAinda não há avaliações
- Visual Ergonomics at Work and Leisure: Paying It ForwardDocumento2 páginasVisual Ergonomics at Work and Leisure: Paying It ForwardDiego A Echavarría AAinda não há avaliações
- Can The Office Environment Stimulate A Manager's Creativity?Documento14 páginasCan The Office Environment Stimulate A Manager's Creativity?Diego A Echavarría AAinda não há avaliações
- SSL Trajectories Proc IEEEDocumento18 páginasSSL Trajectories Proc IEEEDiego A Echavarría AAinda não há avaliações
- Synergies Between Ergoecology and Green Ergonomics: A Contribution Towards A Sustainability Agenda For HFEDocumento6 páginasSynergies Between Ergoecology and Green Ergonomics: A Contribution Towards A Sustainability Agenda For HFEDiego A Echavarría AAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- E3sconf hrc2018 02017Documento5 páginasE3sconf hrc2018 02017Diego A Echavarría AAinda não há avaliações
- Posture: Good Posture Definition & MeaningDocumento13 páginasPosture: Good Posture Definition & Meaningweak manAinda não há avaliações
- Common Yoga Protocol - pdfiYD 2019Documento46 páginasCommon Yoga Protocol - pdfiYD 2019santosh_sbsAinda não há avaliações
- ASD - When Sitting Correctly MattersDocumento4 páginasASD - When Sitting Correctly MattersEduardo DiestraAinda não há avaliações
- Posture and Body MechanicsDocumento12 páginasPosture and Body MechanicsJohn Noah AguilarAinda não há avaliações
- Ceramic Tips ExercisesDocumento4 páginasCeramic Tips Exercisesapi-352404013Ainda não há avaliações
- Osg Catalogue March 2021Documento72 páginasOsg Catalogue March 2021Ritvik KhuranaAinda não há avaliações
- Hawes 2003Documento12 páginasHawes 2003Karibeños San JavierAinda não há avaliações
- Chapter 5Documento14 páginasChapter 5Monica ViceraAinda não há avaliações
- The Importance of Non-Exercise Movement For Longevity: by Dr. MercolaDocumento4 páginasThe Importance of Non-Exercise Movement For Longevity: by Dr. MercolaSellappan MuthusamyAinda não há avaliações
- POSTUREDocumento46 páginasPOSTURENikks BoradeAinda não há avaliações
- Eugene Rawls - Handbook of Yoga For Modern Living PDFDocumento177 páginasEugene Rawls - Handbook of Yoga For Modern Living PDFElla Miu100% (1)
- Developing Good Grooming Practices and Body Care: What Is Personal Hygiene?Documento9 páginasDeveloping Good Grooming Practices and Body Care: What Is Personal Hygiene?Cathy GabiaAinda não há avaliações
- Sagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsDocumento5 páginasSagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsVizaAinda não há avaliações
- Primal Academy For Sports Science: Choose ONE of The Following AnswersDocumento27 páginasPrimal Academy For Sports Science: Choose ONE of The Following AnswerspraveenAinda não há avaliações
- Use of Different Types of Comfort/Support DevicesDocumento20 páginasUse of Different Types of Comfort/Support DevicesConvalescent Nursing HomeAinda não há avaliações
- Posture PDFDocumento30 páginasPosture PDFSairelle Sordilla Obang100% (1)
- Elvic Floor Muscle Activity in Different Sitting Postures in Continent and Incontinent Women - Sa - 0Documento7 páginasElvic Floor Muscle Activity in Different Sitting Postures in Continent and Incontinent Women - Sa - 0Pollyana Furtado JunqueiraAinda não há avaliações
- Dynamic Neuromuscular StabilizationDocumento20 páginasDynamic Neuromuscular StabilizationAnanda Kartika P.100% (3)
- Pelvic SwayDocumento2 páginasPelvic SwaywalterAinda não há avaliações
- Structure and Function of The Vertebral ColumnDocumento60 páginasStructure and Function of The Vertebral ColumnJohn DoeAinda não há avaliações
- Prelim Notes (Pe)Documento10 páginasPrelim Notes (Pe)secretAinda não há avaliações
- Zona Neutra Wallden, 2009Documento12 páginasZona Neutra Wallden, 2009anon_861143750Ainda não há avaliações
- Degenerative ScoliosisDocumento8 páginasDegenerative ScoliosisAnonymous 2q4eg3hgEvAinda não há avaliações
- Total Postural Reprogramming: 3rd EditionDocumento21 páginasTotal Postural Reprogramming: 3rd EditionXXXXXXXX50% (2)
- Programa Kineto EngDocumento3 páginasPrograma Kineto EngDeilePhila OanaAinda não há avaliações
- The 5 Routines - China Soaring Crane Qigong (CSCQ)Documento3 páginasThe 5 Routines - China Soaring Crane Qigong (CSCQ)gabyk68Ainda não há avaliações
- Perkins 1998Documento10 páginasPerkins 1998Emma AzAinda não há avaliações
- Progressing From The Hang Power Clean To The Power.8Documento9 páginasProgressing From The Hang Power Clean To The Power.8Charles VerschurenAinda não há avaliações
- Exercises To Correct Forward Neck PostureDocumento7 páginasExercises To Correct Forward Neck PostureIan Dale100% (2)
- Pilates and The Powerhouse II PDFDocumento9 páginasPilates and The Powerhouse II PDFviboramorAinda não há avaliações
- Horse Care 101: How to Take Care of a Horse for BeginnersNo EverandHorse Care 101: How to Take Care of a Horse for BeginnersNota: 4 de 5 estrelas4/5 (5)
- Lead with Your Heart: Lessons from a Life with HorsesNo EverandLead with Your Heart: Lessons from a Life with HorsesNota: 4 de 5 estrelas4/5 (8)
- Project Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroNo EverandProject Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroNota: 5 de 5 estrelas5/5 (9)
- The Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationNo EverandThe Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationAinda não há avaliações
- The Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingNo EverandThe Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingAinda não há avaliações
- The Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenNo EverandThe Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenNota: 4.5 de 5 estrelas4.5/5 (49)