Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Role of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestDocumento3 páginasRole of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestsimbawulaAinda não há avaliações
- Daftar PustakaDocumento5 páginasDaftar PustakaGeraldo Primaman CoffeeAinda não há avaliações
- Lec19 PDFDocumento11 páginasLec19 PDFsyakiraAinda não há avaliações
- Asymp Bacteriuria A.almuhrijDocumento24 páginasAsymp Bacteriuria A.almuhrijAbdulRahman AlMuhrijAinda não há avaliações
- ICDXDocumento43 páginasICDXAris NurzamzamiAinda não há avaliações
- CSF & Body FluidDocumento42 páginasCSF & Body FluidlopaAinda não há avaliações
- EAP Foundation What Is Ac WritingDocumento6 páginasEAP Foundation What Is Ac WritingColin RobertsAinda não há avaliações
- Antimicrobial Susceptibility Testing - Primer For CliniciansDocumento20 páginasAntimicrobial Susceptibility Testing - Primer For Cliniciansdipzhit100% (1)
- اسئلة الجلدية لهيئة التخصصات السعودية PDFDocumento24 páginasاسئلة الجلدية لهيئة التخصصات السعودية PDFDrhisham AttiaAinda não há avaliações
- Q&A: H1N1 Pandemic Influenza - What's New?: Question & Answer Open AccessDocumento6 páginasQ&A: H1N1 Pandemic Influenza - What's New?: Question & Answer Open AccesskarpanaiAinda não há avaliações
- Tarea 4 de Ingles 4 UNIVERSIDAD ABIERTA PARA ADULTOS UAPADocumento6 páginasTarea 4 de Ingles 4 UNIVERSIDAD ABIERTA PARA ADULTOS UAPAAlexander Polanco50% (2)
- Assessing The IntegumentaryDocumento73 páginasAssessing The IntegumentaryHelena Meurial HilkiahAinda não há avaliações
- Disorders of Brain Function (Neurological) 3Documento12 páginasDisorders of Brain Function (Neurological) 3Cres Padua QuinzonAinda não há avaliações
- VcoDocumento17 páginasVcoLourdes EsperaAinda não há avaliações
- Pharyngitis Case ReportDocumento4 páginasPharyngitis Case ReportMelissa TiofanAinda não há avaliações
- Pictorial Key of Animal Publich Health PDFDocumento197 páginasPictorial Key of Animal Publich Health PDFWahyu RainAinda não há avaliações
- Dracunculiasis (Guinea Worm Disease) : Eradication Without A Drug or A VaccineDocumento29 páginasDracunculiasis (Guinea Worm Disease) : Eradication Without A Drug or A VaccineDina sayunaAinda não há avaliações
- Local LiteratureDocumento3 páginasLocal LiteratureAnngelyn Joy Santos67% (3)
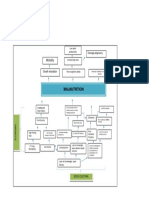
- Problem Tree Analysis MalnutritionDocumento1 páginaProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Malawi Public Health ActDocumento63 páginasMalawi Public Health ActKondwani AndreahAinda não há avaliações
- Infection Illness Exam Mid ReviewDocumento33 páginasInfection Illness Exam Mid ReviewJes CmtAinda não há avaliações
- Dengue FeverDocumento18 páginasDengue FeverJelaine CEAinda não há avaliações
- Expression Ready RFP Retroviral ParticlesDocumento1 páginaExpression Ready RFP Retroviral ParticlesAlleleBiotechAinda não há avaliações
- Lecture Notes On Public HealthDocumento342 páginasLecture Notes On Public Healthredroseeeeee67% (3)
- ISR Project - Water Scarcity in MaharashtraDocumento38 páginasISR Project - Water Scarcity in MaharashtraSuraj0% (2)
- Heroin in ColoradoDocumento62 páginasHeroin in ColoradoMichael_Lee_RobertsAinda não há avaliações
- Main PDFDocumento4 páginasMain PDFNadya Dwi PuspitasariAinda não há avaliações
- Teqnique of PharaprasingDocumento2 páginasTeqnique of PharaprasingMahesa NasutionAinda não há avaliações
- Resume Tutorial A Skenario 1 Blok 14Documento74 páginasResume Tutorial A Skenario 1 Blok 14Istaz MaulanaAinda não há avaliações
- Sequelae of Dental CariesDocumento20 páginasSequelae of Dental Cariesimi4100% (2)