Você também pode gostar
- Determinants For Oral Hygiene and Periodontal Status Among Mentally Disabled Children and AdolescentsDocumento7 páginasDeterminants For Oral Hygiene and Periodontal Status Among Mentally Disabled Children and AdolescentsHusna LathiifaAinda não há avaliações
- Definition and Classification of CPDocumento45 páginasDefinition and Classification of CPMichealowen BabygoalAinda não há avaliações
- Pink and White Bordered Floral Friendship Day CardDocumento1 páginaPink and White Bordered Floral Friendship Day CardHusna LathiifaAinda não há avaliações
- Ventilator Management - StatPearls - NCBI BookshelfDocumento13 páginasVentilator Management - StatPearls - NCBI BookshelfHusna LathiifaAinda não há avaliações
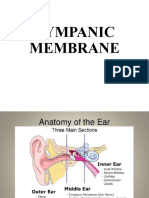
- Tympanic Membrane 1Documento16 páginasTympanic Membrane 1Husna LathiifaAinda não há avaliações
- Presentation 4Documento23 páginasPresentation 4Husna LathiifaAinda não há avaliações
- Logo RshsDocumento1 páginaLogo RshsHusna LathiifaAinda não há avaliações
- Mortality Rate of Patients With Tuberculosis-Destroyed Lung Who Underwent Pulmonary Resection Evidence Based Case ReportDocumento7 páginasMortality Rate of Patients With Tuberculosis-Destroyed Lung Who Underwent Pulmonary Resection Evidence Based Case Reportatls jakartaAinda não há avaliações
- 1.analysis of Relationship Among The Functional ClassificationDocumento5 páginas1.analysis of Relationship Among The Functional ClassificationHusna LathiifaAinda não há avaliações
- Sarcopenic Dysphagia. A Narrative ReviewDocumento7 páginasSarcopenic Dysphagia. A Narrative ReviewHusna LathiifaAinda não há avaliações
- Mirzaei2018 PDFDocumento7 páginasMirzaei2018 PDFHusna LathiifaAinda não há avaliações
- Effects of Foot Orthoses With Medial Arch Support and Lateral Wedge On Knee Adduction Moment in Patients With Medial Knee OsteoarthritisDocumento8 páginasEffects of Foot Orthoses With Medial Arch Support and Lateral Wedge On Knee Adduction Moment in Patients With Medial Knee OsteoarthritisHusna LathiifaAinda não há avaliações
- Toorthj 6 544 PDFDocumento4 páginasToorthj 6 544 PDFHusna LathiifaAinda não há avaliações
- Core Strength Training For Patients With Chronic Low Back PainDocumento4 páginasCore Strength Training For Patients With Chronic Low Back PainHusna LathiifaAinda não há avaliações
- Functional Performance Testing in Athletes With Functional Ankle InstabilityDocumento10 páginasFunctional Performance Testing in Athletes With Functional Ankle InstabilityHusna LathiifaAinda não há avaliações
- LEAPS Fugl-Meyer InstructionsDocumento17 páginasLEAPS Fugl-Meyer InstructionsDaniele Bertolo100% (1)
- Chapter 4B - Upper Extremity Post Stroke - 0Documento22 páginasChapter 4B - Upper Extremity Post Stroke - 0Giga Hasabi AlkaraniAinda não há avaliações
- A Randomized Trial Comparing Cardiac Rehabilitation To Standard of Care For Adults With Congenital Heart DiseaseDocumento9 páginasA Randomized Trial Comparing Cardiac Rehabilitation To Standard of Care For Adults With Congenital Heart DiseaseHusna LathiifaAinda não há avaliações
- Ham D PDFDocumento1 páginaHam D PDFRabiatul AdawiyahAinda não há avaliações
- Spasticity Lit. Reveiw 2010Documento36 páginasSpasticity Lit. Reveiw 2010lewienAinda não há avaliações
- Laryngeal Motor Cortex and Control of Speech in Humans - Simonyan 2011Documento17 páginasLaryngeal Motor Cortex and Control of Speech in Humans - Simonyan 2011Maite CassanovaAinda não há avaliações
- Konstipasi ICUDocumento7 páginasKonstipasi ICUHusna LathiifaAinda não há avaliações
- Patfis Valvular Heart DiseaseDocumento1 páginaPatfis Valvular Heart DiseaseHusna LathiifaAinda não há avaliações
- Tmi Knee PfpsDocumento1 páginaTmi Knee PfpsHusna LathiifaAinda não há avaliações
- Wartegg Test PDFDocumento1 páginaWartegg Test PDFHusna LathiifaAinda não há avaliações
- 8 Non Structural Misalignments of Body Posture in The Sagittal PlaneDocumento14 páginas8 Non Structural Misalignments of Body Posture in The Sagittal PlaneHusna LathiifaAinda não há avaliações
- Comments, Opinions, and ReviewsDocumento7 páginasComments, Opinions, and ReviewsHusna LathiifaAinda não há avaliações
- Manual Therapy: Theresa Helissa Nakagawa, Carlos Dias Maciel, F Abio Viadanna Serr AoDocumento5 páginasManual Therapy: Theresa Helissa Nakagawa, Carlos Dias Maciel, F Abio Viadanna Serr AoHusna LathiifaAinda não há avaliações
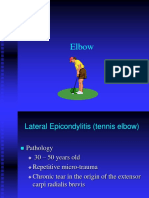
- Elbow, Wrist, HandDocumento47 páginasElbow, Wrist, HandHusna LathiifaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- CVADocumento27 páginasCVAMafe Campo100% (3)
- Management of Stroke PDFDocumento6 páginasManagement of Stroke PDFtarmo angsanaAinda não há avaliações
- CCT - MeaningDocumento10 páginasCCT - Meaningmandeep axonAinda não há avaliações
- Nursing 350 Reflection PaperDocumento7 páginasNursing 350 Reflection Paperapi-2518349340% (1)
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 58Documento11 páginasMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 58sarasjunkAinda não há avaliações
- HESI Case Study Older Adult With StrokeDocumento2 páginasHESI Case Study Older Adult With StrokeAna Bienne100% (1)
- First Aid ManualDocumento68 páginasFirst Aid ManualAntonio Bernard100% (1)
- Jama Kuramatsu 2019 Oi 190098Documento12 páginasJama Kuramatsu 2019 Oi 190098HeliHiAinda não há avaliações
- Stroke Risk Factors in WomenDocumento7 páginasStroke Risk Factors in WomenJosueAinda não há avaliações
- Peripheral Artery DiseaseDocumento45 páginasPeripheral Artery DiseaseIchwan ZuantoAinda não há avaliações
- Aging Changes in The Nervous SystemDocumento4 páginasAging Changes in The Nervous SystemSamira MusayevaAinda não há avaliações
- DokumenDocumento4 páginasDokumenFkep2015Ainda não há avaliações
- Cohort Profile: The Framingham Heart Study (FHS) : Overview of Milestones in Cardiovascular EpidemiologyDocumento14 páginasCohort Profile: The Framingham Heart Study (FHS) : Overview of Milestones in Cardiovascular EpidemiologyAtikah Nur AmalinaAinda não há avaliações
- IM NotesDocumento74 páginasIM NotesRashed ShatnawiAinda não há avaliações
- Perception and CoordinationDocumento32 páginasPerception and CoordinationFerdie Marcial B. AureaAinda não há avaliações
- @MedicalBooksStoreS 2017 Acute IschemicDocumento273 páginas@MedicalBooksStoreS 2017 Acute IschemicAditya Perdana Dharma Wiguna100% (1)
- Hypertonic Saline Versus Mannitol For The Treatment of Elevated Intracranial PressureDocumento6 páginasHypertonic Saline Versus Mannitol For The Treatment of Elevated Intracranial PressureSimone RibeiroAinda não há avaliações
- Dual Antiplatelet Therapy Vs Alteplase For Patients With Minor NondisablingDocumento10 páginasDual Antiplatelet Therapy Vs Alteplase For Patients With Minor Nondisablingbetongo Bultus Ocultus XVAinda não há avaliações
- Golf Croquet Refereeing Manual - Croquet AustraliaDocumento78 páginasGolf Croquet Refereeing Manual - Croquet AustraliaSenorSushi100% (1)
- Effectiveness of The Motor Relearning ApproachDocumento5 páginasEffectiveness of The Motor Relearning ApproachZahid MehmoodAinda não há avaliações
- Ayeni MotunrayoDocumento5 páginasAyeni Motunrayoayenimotunrayo40Ainda não há avaliações
- Rehabilitation After Stroke PDFDocumento8 páginasRehabilitation After Stroke PDFBetaAinda não há avaliações
- Problem in NeurologyDocumento25 páginasProblem in NeurologyMohd Afiq AizuddinAinda não há avaliações
- Clinical Decision Making To Determine Need For Medical ReferralDocumento12 páginasClinical Decision Making To Determine Need For Medical ReferralaroobaAinda não há avaliações
- Stroke 2005 Wojner Alexandrov 1512 8Documento8 páginasStroke 2005 Wojner Alexandrov 1512 8Kevin LiputraAinda não há avaliações
- Oral Anticoagulation in The Elderly and Frail: Rupert M. Bauersachs Joerg HeroldDocumento10 páginasOral Anticoagulation in The Elderly and Frail: Rupert M. Bauersachs Joerg Herold90STRATOVARIUS90Ainda não há avaliações
- CHBP Progress NoteDocumento1 páginaCHBP Progress NoteNelson R. PouAinda não há avaliações
- The Golden Hour of Acute Ischemic StrokeDocumento22 páginasThe Golden Hour of Acute Ischemic StrokeGiao MauAinda não há avaliações
- What Is Cerebral Vascular DiseaseDocumento2 páginasWhat Is Cerebral Vascular DiseasejbvaldezAinda não há avaliações
- A Modified Anatomical-Functional-Rope (Af-Rope) Score Improves Patient Selection For Patent Foramen Ovale ClosureDocumento4 páginasA Modified Anatomical-Functional-Rope (Af-Rope) Score Improves Patient Selection For Patent Foramen Ovale ClosureDessytha NathaniaAinda não há avaliações