Escolar Documentos
Profissional Documentos
Cultura Documentos
HILLSLEY Et Al-1993-Pacing and Clinical Electrophysiology
Enviado por
Marcelo AViDireitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
HILLSLEY Et Al-1993-Pacing and Clinical Electrophysiology
Enviado por
Marcelo AViDireitos autorais:
Formatos disponíveis
Is the Second Phase of a Biphasic Defibrillation
Waveform the Defihrillating Phase?
RUSSELL E. HILLSLEY, ROBERT G. WALKER. DAVID K. SWANSON,
DENNIS L. ROLLINS. PATRICK D. WOLF, WILLIAM M. SMITH,
and RAYMOND E. IDEKER
From the Departments of Medicine and Pathology. Duke University Medical Center, and the
Engineering Research Center for Emerging Cardiovascular Technologies of the School of
Engineering. Durham, North Carolina
HILLSLEY, R.E., ET AL.: IS the Second Phase of a Biphasic Defihrillation Waveform the DePihrillating
Phase? Why some biphasic waveforms defibrillate with lower energies Ihan monophasic waveforms of
similar duration is unknown. One hypothesis is that the first phase of a hiphasic waveform acts as a
conditioning, hyperpolarizing prepulse to prepare for defihri/Iafion by a second depolarii^ing phase. To
test whether the second phase of a biphasic waveform is the de/ibriiiating phase, three monophasic
wave/arms, an ascending ramp (AJ, a square wove (SJ, and a descending ramp (D), were compared to
three biphasic waveforms with A, S, or D in the first phase fbiphasic first phasej and three hiphasic
waveforms with A, S, or D in the second phase (biphasic second phasej. Two defibrilicition thresholds
for each ivaveform were performed in IS open chest pigs and mean defibril/ation threshoJds were com-
pared. In nine pigs 16-msec monophasic and 16/16-msec biphasic waveforms were ranked hy mean
current and energy at defibrilJation threshold. The ranks were the same for monophasic and hiphasic
secondphase waveforms: for mean current A < S = D and for energy A < S < D. The ranks were different
for the biphasic first phase ivaveforms: far mean current S < A = D and for energy S < A = D. Aithough
ranks for the ]G-msec monophasic ivaveforms matched those for the 16/16-msec hiphasic second phase
waveforms, the biphasic ivaveforms had higher mean currents and energies at defihriilation threshoid.
in nine pigs defihrilJation thresholds for 6-msec monophasic and 6/6-msec biphasic ivaveforms were
ranked. For mean current the ranks were monophasic: A < S ^ D: biphasic first phase: A = S = D;
and biphasic second phase: S ^ D < A. For energy the ranks were monophasic: A = S < D; hiphasic
first phase: A = S = D: and hiphasic second phase; S = D < A. Thus, ranks for the 6-nisec monophasic
waveforms di/feredfrom those for the 6/6-msec biphasic second phase waveforms. For 16/16-msec bipha-
sic waveforms, Jess effective for defihriJJation than corresponding 16-msec monophasic waveforms, these
results support the hypothesis that the second phase of a biphasic waveform defihriJJates since the
defihriilation efficacy of a 16/16-msec biphasic waveform is reiated to the defibriiiation efficacy of its
second phase waveshape. However, for cJinicaiJy usefuJ 6/6-msec biphasic waveforms, more effective
for defibriJIation than 6-msec monophasic waveforms, (he hypothesis is not supported because the ability
of a 6/6-msec biphasic waveform to defibriJJate is unreJated to the defibrilJation efficacy of its second
phase waveshape. (PACE, Vol. 16, July 1993, Part IJ
ventricuJarfibriJJation, defibriJJation, biphosic shocks, sudden cardiac death
Supported in part by the National Institutes of Health research
grants HL-42760, HL-44066. HL-28429, and HL-33637, The Na- Introduction
tional Science Foundation Engineering Research Center Grant
CDR-8622201, and by Cardiac Pacemakers, Inc. and Physio- Implantable cardioverter defibrillators may
Control Corporation. use either monophasic waveforms or biphasic
Address for reprints: Russell E. Hillsley, M.D., Box 31046, Duke waveforms with a second phase of opposite polar-
University Medical Ctr., Durham, NC 27710. Fax: (919) 660-
5405. ity to the first. Many biphasic waveforms have
Received September 24, 1992; revision January 12. 1993; ac-
been observed to defibriliate with lower current
cepted February 5, 1993. and energy than monophasic waveforms of similar
PACE. Vol. 16 July 1993, Part I 1401
HILLSLEY. ET AL.
duration altbough the mechanism is not with tbe National Institutes of Health Guide for
known.'"" Jones et al.'^"'"* hypothesize that tbe the Care and Use of Laboratory Animals."'
first phase of a bipbasic shock acts as a condition-
ing prepulse to reduce tbe threshold for excitation Animal Preparation
or prolongation of refractoriness by the second de-
fibrillating phase. Twenty pigs (25-40 body mass] were preanes-
An implication of this hypothesis is that the thetized witb ketamine (25 mg/kg) and acepromaz-
second pbase of the biphasic waveform is acting ine (0.5 mg/kg), intramuscularly. Subsequently,
similarly to a monophasic waveform. To test this anesthesia was maintained with pentoharbital (8
implication, three monopbasic waveforms of dif- mg/kg initial intravenous dose followed by a con-
fering defihrillation efficacy were chosen and used tinuous intravenous infusion of 0.05 mg/kg per
as the first or second pbase of biphasic waveforms min). Succinylcholine (1.5 mg/kg initial intrave-
with each phase equal in duration to tbat of the nous dose then 0.5 mg/kg intravenously every 20
monophasic waveforms. The goal was to see if min) was used to provide adequate muscle relaxa-
varying the waveshape of the second phase of a tion. The pigs were intubated with a cuffed endo-
hiphasic waveform caused changes in defihrilla- tracheal tube and ventilated with room air and ox-
tion efficacy similar to those produced hy varying ygen through a respirator [Harvard Apparatus,
the waveshape of a monophasic waveform. Inc., South Natick, MA. USA). A femoral arterial
line was inserted and systemic pressure was con-
Scbuder et al,'^ found that ascending ramps tinuously displayed. Rectal temperature was mon-
of long duration defihrillated more effectively than itored continuously and maintained within nor-
descending ramps. Thus, the initial monopbasic mal limits. Arterial blood samples were drawn
waveforms used were an ascending ramp, a de- every 60 minutes for determination of pH, partial
scending ramp, and a square wave, each 16 msec pressure of oxygen (pO:;). and serum electrolytes.
in duration: and 16/16-msGc biphasic shocks with Normal saline with dextrose was continuously in-
tbe waveforms above in the second phase and a fused and supplemented as needed to maintain pH
square wave of the same mean current but oppo- and electrolytes within normal ranges. Electrocar-
site polarity in the first phase. Bipbasic shocks diographic leads were applied for continuous
with the above monophasic waveforms in tbe first monitoring.
phase and a square wave in the second phase were
also tested to see if varying the first phase of the The chest was opened by median sternotomy
hiphasic had a different effect. Since the duration and the pericardial sac opened to expose the heart.
of biphasic waveforms commonly used in avail- Large, contoured, stainless steel electrodes were
able defibrillators is usually much shorter tban 32 then sutured to the heart for delivering defibrilla-
msec and since the observations made at these tion shocks. The right ventricular epicardial elec-
shock durations may not also apply to shorter trode was the cathode for monophasic shocks and
shocks, the second part of tbe study examined de- fur the phase with variable waveshape in the bi-
fibrillation with the same waveshapes but a phasic shocks: the left ventricular epicardial elec-
shorter duration: 6-msec monophasic and 6/6- trode was of tbe opposite polarity.
msec bipbasic waveforms.
Defibrillation Protocol
Methods Ventricular fibrillation was induced by 60-Hz
alternating current delivered lor approximately 1
This study consisted of two similar hut dis- second through two wires sutured to the epicar-
tinct protocols, descrihed as part I and part II dium. Defihrillation waveforms were created by a
helow. Part 1 measured defibrillation thresholds custom-built, constant-current waveform genera-
for long (16/16 msec) hiphasic waveforms wbile tor (Cardiac Pacemakers. Inc.. St. Paul. MN, USA).
part II determined defihrillation thresholds for Fihrillation was sustained for 15 seconds before
shorter (6/6 msec) biphasic waveforms. The com- defibrillation was attempted. A failed defibrilla-
mon portions of the protocol are descrihed first. tion was followed hy a rescue shock of higher en-
All pigs were treated and cared for in accordance ergy than the failed shock and delivered hy a 150-
1402 July 1993, Part 1 PACE, Vol. 16
EFFECT OF WAVESHAPE ON DEFIBRILLATION
[JLF defibrillator (HVS-02, Ventritex. Inc., Sun- waveforms, an ascending ramp, a square wave,
nyvale, CA, USA). During each attempted defibril- and a descending ramp, were each 16 msec in du-
lation the applied current and voltage across the ration. The biphasic waveforms were all 32 msec
heart were sampled at 20 kHz by a Data Precision in duration, 16 msec in each phase. The mean cur-
6100 waveform analyzer [Data Precision, Inc., rent of the first phase of the biphasic was set equal
Danvers, MA, USA). Signal analysis software to the mean current of the second phase. Three
within the analyzer was used to obtain the imped- of the biphasic waveforms were composed of the
ance and energy measurements. The output of the monophasic waveforms above in phase one with
waveform analyzer was sent to a computerized da- a square wave of opposite polarity in phase two
tafile [Sun Microsystems, Inc., Mountain View, [biphasic first phase). The other three biphasic
CA, USA) and stored. At least 4 minutes were al- waveforms contained the monophasic waveforms
lowed for the animal to recover after each fibrilla- in phase two with a square wave of opposite polar-
tion-defibrillation episode. ity in phase one (biphasic second phase).
The defibriliation threshold was defined as
Part I the lowest current and energy that achieved defi-
brillation. The initial current was the mean cur-
Nine different defibrillation waveforms were rent at defibrillation threshold for that waveform
tested (Fig. 1) in 11 pigs. The three monophasic in the previous animals. If a defibrillation shock
Ascending Ramp Square Descending Ramp
was successful, the mean current of the monopha-
(A) (S) (D) sic or both phases of the biphasic shock was de-
Monophasic creased by 0.4 A, and a repeat attempt at defibrilla-
tion was made. This procedure was repeated until
an unsuccessful shock occurred; then, the mean
current was increased by 0.2 A, and a final defibril-
Biphasic - First Phase lation attempt was made. If the initial defibrilla-
tion shock failed, the mean current was increased
t 0.4 A, and a repeat attempt at defibrillation was
2a made. This procedure was repeated until a suc-
cessful defibrillation occurred; then, the mean cur-
rent was decreased by 0.2 A for the final defibrilla-
f tion attempt.
Biphasic - Second Phase Two sets of nine defibrillation thresholds
t were performed for each animal. The defibrillation
2a threshold for each waveform was determined in
random order in each set. Two animals died dur-
1 f f
ing the second set of defibrillation thresholds;
only the first complete set of defibrillation thresh-
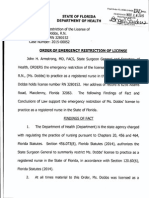
Figure 1. Ninf! r;urrenf waveforms used in parf 1. The olds was included for those animals. Two animals
three monophasic waveforms are each 16 msec in dura- were excluded from analysis: one died before com-
tion. The six hiphasic waveforms are 32-msec total du- pleting a single set of defibrillation thresholds; in
ration and 16 msec in each phase. For the biphasic-/irst the other animal the electrodes were inadvertently
phase waveforms (he monophasic waveform was used used in reverse polarity throughout the exper-
as the first phase wilh the second phase a square wave iment.
wilh opposile polarity. For the biphasic-second phase
waveforms the monophasic waveform was used as the
second phase wilh a square wave of opposite polarity Part II
preceding il. In all the hiphasic waveforms the mean
current of the first phase equah the mean current of tbe Nine different defibrillation waveforms were
second phase. The peak current in each phase of the tested (Fig. 2) in nine pigs. The three monophasic
biphasic waveforms is represented as multiples of the waveforms, an ascending ramp, a square wave,
symbol a. and a descending ramp, were each 6 msec in dura-
PACE, Vol. 16 July 1993, Part I 1403
HILLSLEY, ET AL.
Ascending Ramp Square Descending Ramp by 0.4 A, and the mean current of the second phase
(A) (S) (D) was changed by 0.2 A. After a transition from suc-
cess to failure or failure to success, the final change
in mean current was 0.2 A for the first phase hut
Monophasic 0.1 A for the second phase.
Two sets of nine defibrillation thresholds
were determined in each pig. As in part 1. the defi-
brillation threshold for each waveform was deter-
l\ 2a Biphasic - First Phase mined in random order in each set. One animal
died during tho second set of defibrillation thresh-
t olds: only the first complete set of defibriiiation
Biphasic - Second Phase thresholds was included for this animal.
Upon completion of a protocol, the pig was
euthanized by electrically induced fibrillation.
The electrodes were removed and the heart was
Figure 2. Nine currenf waveforms used in porl /I. The
excised and weighed.
Ihref! monophnsic uav'f;/nrm,s QTP. each 6 msec in dum-
Hon. The six biphasir wtn'ejnrms are I2-msec total du- Statistical Analysis
ration and 6 msec in each phase. For Ihe bi phasic-firs I
phase waveforms the monophasic ivavofonn was used
In part I. 16 complete sets of defibrillation
as phase one ivifh tb(; .second phase a square wuve with thresholds were available: two sets from each of
opposite pokirily. For fhe biphasic-second phase wove- seven animals and one set from each of two ani-
forms the monophasic waveform was used as the sec- mals. In part II, 17 complete sets of defibrillation
ond phase wilh a square wave of opposite polarity pre- thresholds were available: two sets from each of
ceding i(. In all (he hiphasic waveforms (he mean eight animals and one set from one animal. For
current oi (he firsl phase was twice the mean curi-enl of each part of the experiment data from ail com-
the second phase. The peak current in each phase of pleted sets of nine defibrillation thresholds, 16
the biphasic waveforms is represented by mu/tiples of sets in part I and 17 sets in part II. were combined
the symbol a. to determine a mean and standard deviation for
each waveform. Repeated measures analysis of
variance with the Student-Newnian-Keul's test
tion. The biphasic waveforms were all 12 msec, (SAS Institute. Inc.. Cary, NC. USA) was used to
6 msec per phase, To simuiato the most effective compare the three monophasics and produce a
biphasic waveforms studied and currently in use rank order hy mean current and energy. The same
in available defibriliators, the mean current of the procedure was followed to produce rank orders for
first jjhase of the biphasic was set to twice the the three biphasic first phase waveforms and rank
mean current ofthe second phase.^ •*•"'" As in part orders for the three biphasic second phase wave-
I, three biphasics were composed of the monopha- forms. The null hypothesis was rejected for P <
sics above in phase one and a square wave of oppo- 0.05 and P < 0.05 was required for each compari-
site polarity in phase two (biphasic first phase). son to be statistically significant.
The other three biphasics contained the monopha-
sics above in phase two and a square wave with
opposite polarity in phase one (biphasic second Results
phase).
The defibrillation threshold was defined simi- Parti
larly and an identical protocol to that in part I was The mean heart weight was 178 ± 19.2 g for
followed for the monophasic waveforms. Since the the nine pigs. Figure 3 depicts the mean energy at
mean current of the first phase of the biphasic defihrillation threshold for each waveform in each
waveforms was twice the mean current of the sec- of the nine pigs. After combining the data from all
ond phase, initially during defibrillation testing 16 sets of defibrillation thresholds in nine pigs,
the mean current of the first phase was changed the mean current and energy at defibrillation
1404 luly 1993. Part I PACE. Vol. 16
EFFECT OF WAVESHAPE ON DEFiBRItXATION
80 Monophasic
Q.—o Ascending Ramp
a — • Square
O—O Descending Ramp
Biphasic - First Phase
G- -O Ascending Ramp
60 Q-- D Square / \
O - O Descending Ramp / \
Biphasic - Second Phase 1 «> ^ o. if
•' ••• /I
O- -G Ascending Hamp tl
,'O ••, //
Q—E] Square / ,'H\ \ ,,
;'•
•,
'••,
••,'/
f.
<>—0 Descending Ramp ,-'•' P-\ \ .f •/ ••
-••'•' / Nft
40 ••'/ \ \ \ V
x
c / /•
)• ,•• / /
LU ^ . '•••.
y /
\\^' / /
'•\\ l\i '^ \^\ ! ^1
20
^^ / .0' 3
''•'.''<> i ,'•:
W / •
/ \
& \\ VS
'• It
y ^ y\;'' /•''-' ,0 -^
^ ^ ^ ^ ^ ^
G— e^
n
G- e- —©"^
J L . 1 1
>—^1^^
5
Animal
Figure 3. De/ibrilJalion threshold energy/or Ihe nine lG-msec monophasic OT 16/16-msec bipha-
sic mi ve/onns te.fited in parf f ploflod/or ecich animcil. For seven animnis (he energies represent
the mean of two de/ibri/I(j(ion threshulds; in two animah only onv. de/ibrilJulion threshold is
represenled.
threshold were determined and are given in Tables the corresponding monophasic waveforms (P <
I and I! for the nine long waveforms. The ranks for 0.05).
tho monophasic, the biphasic first phase, and the For the monophasic waveforms the ascending
biphasic second phase waveforms are given in ramp had the lowest mean current and energy at
Table III (duration 16 msec). The ranks were hased defibrillation threshold. By contrast the descend-
on the first phase energy for the bipiiasic first ing ramp had the highest mean current and energy
phase waveforms and the second phase energy for at defibrillation threshold. The square wave was
the biphasic second phase waveforms. For the bi- not different from the descending ramp by mean
phasic waveforms the mean current and energy at current but was intermediate between the ascend-
defihrillation threshold were higher than those for ing ramp and descending ramp by energy.
Table 1.
Mean Current ± Standard Deviation (Amps) at Defibrillation Threshoid for 16 msec Monophasics
and 16/16 msec Biphasics
Waveform Ascending Ramp Square Descending Ramp
Monophasic 2.37 ± 0,88 3,43 ± 0,53 3,46 ± 0,82
Biphasic-first phase 4.54 ± 1,15 3.60 ± 1.33 4.79 ± 1.33
Biphasic-second phase 2,65 ± 0.86 4.14 ± 1.52 4.41 ± 1.52
PACE, Vol. 16 July 1993. Part ! 1405
HtLLSLEY, ET AL.
Table 11.
Energy ± Standard Deviation (Jouies) at Defibriliation Threstioid for 16 msec Monophasics
and 16/16 msec Biphasics
Ascending Ramp Square Descending Ramp
Monopbasic 5.48 :t 3.78 8.41 ± 2.09 10.4 + 4.18
Biphasic-first phase
First phiase energy 18.0 -t 7.88. 9.75 ± 6.26 19.6 ± 9.83
Totai energy 31.3 ^t 13.7 18.7 ± 12.3 34.1 + 17.5
Bipliasic-second phase
Second phase energy 6.19 1- 3.88 12.1 ± 8.40 16.4 ± 11.4
Totai energy 11.6 ir 7.03 25.2 + 16.8 30.4 ± 20.0
The biphasic first phase waveforms ranked threshold for each of the nine short waveforms in
differently from the monophasic waveforms. The each of nine pigs is shown in Figure 4. For the
most effective waveform by mean current and en- combined 17 sets of defibrillation thresholds
ergy was the square wave. The ascending and de- available from nine pigs, the mean current and en-
scending ramps were not different from each other ergy at defibrillation threshold for the nine short
by either criterion. waveforms were determined and are given in Ta-
With the biphasic second phase waveforms, hles IV and V. The ranks for the monophasic, the
the ascending ramp again had the lowest mean biphasic first phase, and the biphasic second
current and energy at defibrillation threshold, As phase waveforms are given in Table III (duration
for the monophasic waveforms, the descending 6 msec). The ranks for the hiphasic first phase
ramp was the worst by mean current and energy waveforms were derived from the mean current
while the square wave matched the descending and energy contained in the first phase, and the
ramp by mean current but was intermediate be- ranks for the biphasic second phase waveforms
tween the ascending and descending ramps by en- were derived from the mean current and energy
ergy. Thus, the ranks for the monophasic wave- in the second phase. Unlike in part L the mean
forms and the biphasic second phase waveforms current and total energy at the defibrillation
were identical and the ranks for the biphasic first threshold for the biphasic waveforms were lower
phase waveforms were different. than for the corresponding monophasics (P <
0.05].
Part II For the monophasic waveforms the ascending
ramp was the most effective by mean current,
The mean heart weight was 170 ± 19.2 g for but by energy the square wave and ascending
the nine pigs. The mean energy at defihrillation ramp were equally effective. By mean current
Table IIL
Rank Orders By Mean Current and Energy
16 msec 6 msec
Duration Mean Current Energy Mean Current Energy
Monophasic A < S - D A< S< D A< S = D A - S < D
Biphasic-first phase S < A - D S < A - D A - S = D A - S - D
Biphasic-second phase A< S - D A < S< D S - D < A S = D < A
1406 July 1993. Part I PACE, Vol.
EFFECT OF WAVESHAPE ON DEFIBRILLATION
Monophatic
G—o Ascending Ramp
15 B—o Square
O—O Descending Ramp
Biphasic - First PhaM
O- o Ascending Ramp
D • Square
O—O Descending Ramp
Biphasic - Second Phase
O- - o Ascending Ramp
10 Q — • Square
0—o Descending Ramp
CD
LU
1 2 3 4 5 6 7 8 9
Animal
Figure 4. Defibrillation threshold energy for tbe nine 6-msec monophasic or 6/6-msec biphasic
waveforms tested in part JI plofled for each animal. For eight nnimaJs Ihe energies represent
the mean af two de/ibrillalion thresholds; in one animal only one defibrilJalion threshold for
each waveform is represented.
and energy the descending ramp was the worst The biphasic second phase waveforms were
waveform. different and the ascending ramp was the least ef-
The biphasic first phase waveforms wero not fective for defibrillation. The square wave and de-
different for either mean current or energy. (P ^ scending ramp were equally effective, and both
0.34 for rejecting the null hypothesis for mean cur- defibrillated better than the ascending ramp. Nota-
rent and P - 0.40 for rejecting the null hypothesis bly, although the 6-msec monophasic ascending
for energy.) ramp was the most efficient at defibrillation, the
Table IV,
Mean Current Standard Deviation (Amps) at Defibrillation Threshold for 6 msec Monophasics
and 6/6 msec Biphasics
Ascending Ramp Square Descending Ramp
Monophasic 3.92 ± 1,07 4.61 ± 1.15 4.66 ± 1.00
Biphasic-first phase
First phase mean current 2.65 ± 0.85 2.86 ± 0.67 2.82 ± 0.77
Both phases mean current 1.90 ± 0.63 2.11 ± 0.51 2.05 ± 0.58
Biphasic-second phase
Second phase mean current 1.63 ± 0.48 1.26 ± 0.33 1.23 ± 0.29
Both phases mean current 2.33 ± 0.69 1.95 ± 0.50 1.78 ± 0.44
PACE. Vol. 16 July 1993. Part I 1407
HILLSLEY, ET AL,
Table V.
Energy ± Standard Deviation (Joules) at Defibriilation Threshold for 6 msec Monophasics
and 6/6 msec Biphasics
Waveform Ascending Ramp Square Descending Ramp
Monophasic 5.16 ± 3.07 5.62 ± 2,70 6.74 + 2.72
Biphasic-first phase
First phase energy 2.43 ± 1.45 2.33 ± 1.04 2.67 ± 1,44
Totai energy 2,75 ± 1.67 2.74 ± 1.26 3.05 + 1,68
Biphasic-second phase
Second phase energy 0,73 ± 0.47 0.36 ± 0,21 0.38 ± 0.21
Total energy 3.31 ± 1.98 2.33 ± 1,17 1.94 ± 1.07
6/6-mset: biphasic with an ascending ramp in the tion. In earlier studies of cardiac stimulation, as-
second phase was the least efficient. This resuit cending ramp waveforms stimulated myocardium
contrasts with that from part I for which the 16- more effectively, with iess energy and charge, tban
msec monophasic ascending ramp and the 16/16- did a square wave or a descending ramp.'^'"
msec biphasic with the ascending ramp in the sec- Tbese results for stimuiation are consistent witb
ond phase were the most efficient monophasic and tbe resuits for defibrillation with monopbasic
hiphasic waveforms, respectively. Thus, the ranks shocks of 6-msec and 16-msec duration. In both
for the 6-msec monophasic waveforms and the 6/ cases tbe descending ramp required the greatest
6-msec hiphasic second phase waveforms were energy for defibrillation. in addition, tbe ascend-
different. ing ramp defibrillated witb lower mean current
tban did tbo square wave or tbe descending ramp
Discussion at hoth durations.
Schuder et al.^^ demonstrated a greater proba-
This study investigated the mechanism of de- bility of successful defibrillation for transthoracic
fibrillation witb biphasic waveforms by defibril- defibrillation witb ascending ramps than descend-
lating with shocks of different waveshapes and de- ing ramps when shock duration was longer than
termining whether the defibrillation efficacy of tbe 16 msec. Unlike in the present study, at shorter
first or second phase of tbe biphasic waveform cor- durations tbe two ramp waveforms appeared simi-
responded to tbat of a monopbasic waveform. For lar in efficacy. However, defibrillating with epicar-
monopbasic waveforms defibriilation efficacy dial electrodes in open cbest pigs may not give tbe
witb ramps and square waves was found to corre- same results as with transthoracic electrodes in
spond to the stimulation efficacy of these wave- calves. In addition, tbe waveforms were not tested
forms in previous studies.^^^'* Short duration (6 in random sequence in tbe calves. Matbematical
msec) monopbasic ascending ramps defibrillated models and experiments witb trapezoidal wave-
better tban square waves or descending ramps. For forms, wbicb approximate ascending and de-
16/16-msec bipbasic waveforms, varying tbe scending ramps, have shown improved defibrilla-
shape of the second pbase produced similar tion efficacy with ascending ramp waveforms. ^^'^^
cbanges in defibrillation efficacy to tbose pro-
duced by varying tbe sbape of a 16-msec mono- The similar results for myocardial stimulation
phasic waveform; this was not true for 6/6-msec and defihrillation with tbese monopbasic
bipbasic waveforms. wavesbapes are consistent witb the hypothesis
tbat monopbasic waveforms defibriliate by excita-
Monophasic Waveforms tion or by prolongation of refractoriness. Tbese
results differ from those witb sbort duration bi-
Scbuder and co-workers^^ first used ascend- phasic sbocks.^'-^^ Sbort biphasic shocks that
ing and descending ramp waveforms for defibrilla- defibrillated more efficiently tban monopbasic
1408 July 1993, Part I PACE, Vol, 16
EFFECT OF WAVESHAPE ON DEFIBRILLATION
waveforms did not excite myocardium or prolong corresponding monophasic waveforms. Thus,
refractoriness as nffoctively. while there is a beneficial interaction between the
two phases of these biphasic waveforms, it does
Biphasic Waveforms not appear to be explained by the ability of the
The results for the 16/16-msec and 6/6-msec second phase to defibrillate in tho same manner
biphasic waveforms were different. For the 16/16- as the monophasic waveform.
msec biphasic shocks defibrillation efficacy was This finding seems reasonable since for the
related to the ability of the second phase shorter 6/6-msec biphasic waveforms the energy
waveshape to defibrillate. An ascending ramp was content of the second phase was significantly less
the most effective 16-msec monophasic waveform than the energy content of the first phase. Typi-
and the most effective second phase for the 16/16- cally, the first phase contained three to four times
msec biphasic waveform; conversely, the descend- the energy of the second phase. This is also true
ing ramp was the least effective for both. This is of clinically useful biphasic waveforms.'*'" It is
consistent with the hypothesis by Jones et al. '^ '•* difficult to view the first phase of these biphasic
that the first phase of the biphasic waveform pre- waveforms as merely a conditioning phase since
pares the heart for defibrillation by the second it contains such a large proportion of the energy.
phase. However, varying the waveshape of the first phase
However, the defibrillation thresholds for the of the 6/6-msec biphasic waveforms did not pro-
16/16-msec biphasic waveforms were greater than duce a significant change in defibrillation efficacy.
those for the 16-msec monophasic waveforms. For Consequently, the increased efficacy of biphasic
example, the 16-msec monophasic ascending waveforms does not appear to result solely from
ramp had a lower mean current and energy at defi- the ability of the first phase to defibrillate in the
brillation threshold than the 16/16-msec biphasic same manner as the monophasic waveform either.
waveform with an ascending ramp in the second Schuder et al.''^ proposed that descending
phase. Since the biphasic waveform is less effec- ramps were ineffective for defibrillation because
tive at defibrillation than the monophasic wave- they tended to produce refibrillation. This hypoth-
form, it is unlikely that the first phase is condition- esis appears consistent with the results for the
ing the myocardium for defibrillation by the sec- longer waveforms; the descending ramp may have
ond phase. The higher defibrillation thresholds been the worst waveform for the second phase be-
with the 16/16-msec biphasic waveforms com- cause it reinduced fibrillation. However, for the
pared with the 16-msec monophasic waveforms shorter waveforms a descending ramp in the sec-
contrasts with the excitation experiments of Jones ond phase was much more efficient for defibrilla-
et al.'^ in which symmetric biphasic stimuli of up tion than was an ascending ramp.
to 40 msec/phase in duration excited chick myo- This study suggests that it is incorrect to refer
cardial cells better than monophasic stimuli equal to the second phase of all biphasic waveforms as
in duration to the second phase of the biphasic the defibrillating pulse''' since the interaction be-
stimuli. In the present study, the addition of the tween the two phases appears complex. Although
first phase made this long waveform less able to for a long (16/16 msec) biphasic waveform, the de-
defibrillate. fibrillation efficacy varied with the shape of the
For the 6/6-msec biphasic shocks, varying the second phase; this was not the case for a shorter
waveshape of the second phase did not produce (6/6 msec) biphasic waveform. This difference in
the same changes in defibrillation efficacy as defibrillation behavior suggests that different
when varying the monophasic waveshapes. The mechanisms may apply to long and short biphasic
ascending ramp, which was efficacious for the 6- waveforms, and that for the shorter 6/6-msec bi-
msec monophasic waveform, was not as effective phasic waveforms the second phase is not the sole
as either a square wave or a descending ramp when defibriliating phase.
inserted into the second phase of the 6/6-msec bi-
phasic waveform. Unlike the 16/16-msec biphasic Optimizing Defibrillation Waveforms
waveforms, these shorter biphasic waveforms de- Selection of the optimal waveshape is impor-
fibrillated with lower current and energy than the tant to the production of an effective implantable
PACE, Vol. 16 |uly 1993. Part I 1409
HILLSLEY, ET AL.
defibrillator. As suggested by prior studies,^' tbe whicb may increase tbe size of tbe implanted defi-
best dofibrillation wavesbape is not reliably pre- brillator.
dicted by tbe wavesbape tbat stimulates myocar- In earlier studies,^-^ biphasic waveforms with
dium most effectively. Ascending ramps bave a second phase shorter than the first phase were
been sbown to stimulate myocardium effectively, more effective tban tbose with a second pbase
and in tbis study monopbasie ascending ramps longer than or equal in duration to the first. How-
and long (16/16 msec) bipbasic waveforms witb ever, the relative duration of the two phases is not
an ascending ramp in tbe second pbase defibrillate tbe only determinant of biphasic efficacy since all
well; however, sbort [6/6 msec) bipbasic wave- the biphasic sbocks compared in this study had
forms witb an ascending ramp in tbe second pbase pbases of equal duration. The long (16/16 msec)
defibrillate poorly. Tbus, tbe cboice of specific biphasic waveforms were not as effective for defi-
monopbasie and bipbasic wavesbapes for defibril- brillation as tbe 16-msec monopbasie waveforms
lation should not be based solely on tbe ability of and, as a result, are not as useful clinically. For tbe
tbe waveform to stimulate but sbould be tested for 6/6-msec bipbasic waveform an ascending ramp in
defibrillation before being used in a device. tbe second pbase is not as effective as a square
Ascending ramps were tbe best 6-msec and wave or a descending ramp for defibrillation.
16-msec monophasic defibrillation waveforms in Since tbe second phase descending ramp and
this study. By constrast, descending ramps were square waves were equally effective, it may be ac-
the least effective while square waves were inter- ceptable to substitute a bigb tilt exponential wave-
mediate in efficacy. Tbus, if a descending ramp is form into the second phase. Such a waveform bas
considered an approximation of a bigb tilt expo- been described.^^' Varying the shape of the first
nential waveform and a square wave is considered phase of tbe 6/6-msec bipbasic waveform had no
the waveform of lowest tilt, then a low tilt expo- significant effect in this study.
nential monophasic waveform sbould be better
tban one with high tilt. The benefit of low tilt
waveforms bas been noted previously,"'' One prac-
tical disadvantage of low tilt waveforms is tbat
Acknoiv/edgmeitts; We thatik Sharon Meltiick. |enny
they require a larger capacitor for generation. Hagler, and EHen Dixon-Tullocn for their technical asshslance.
References
1. Dixon EG. Tang ASL, Wolf PD. et al. Improved de- use of a hiphasic truncated exponential waveform.
fibrillation thresholds with large contoured epiuar- Am Heart J 1989: 117:122-127.
dial electrodes and biphasic waveforms. Circula- 7. Schuder JG, Cold JH, Stoeckle H, et al, Transtho-
tion 1987: 76:1176-1184, racic ventricular defihrillation in the 100 kg calf
2, Tang ASL. Yabe S. Wharton JM, et al. Ventricular with symmetrical one-cycle bidirectional rectan-
defibrillation using biphasic waveforms: The im- gular wave stimuli. IEEE Trans Binmed Eng 1983:
portance of phasic duration, | Am Goll C'ardiol BME-30:415-422,
1989: 13:207-214. 8. Jones IL, Swartz JF, Jones RE. et al. Increasing fi-
3, Feeser SA. Tang ASL, Kavanagh KM. et al. hrillation duration enhances relative asymmetrical
Strength-duration and probability of success hiphasic versus monophasic defihrillator wave-
curves for defihrillation with hiphasic waveforms. form efficacy, Circ Res 1990: 67:376-384.
Circulation 1990: 82:2128-2141. 9. Elaker GC. Schuder JC, McDaniel WC, et al. Superi-
4. Kavanagh KM, Tang ASL, Rollins DL, et al. Com- ority of hiphasic shocks in the defihrillation of
parison of the internal defihrillation thresholds for dogs by epicardial patches and catheter electrodes.
monophasic and double and single capacitor hi- Am Heart J 1989: 118:288-291,
phasic waveforms, ) Am Goll Gardiol 1989: 14: 10, Bardy GH, Ivey TD. Allen MD. et al, A prospective
1343-1349. randomized evaluation of hiphasic versus mono-
5. P'ain ES, Sweeney MB, Franz MR, Improved inter- phasic waveform pulses on defibrillation efficacy
nal defihrillation efficacy with a biphasic wave- in humans. J Am Goll Cardiol 1989: 14:728-733.
form. Am Heart 1 1989: 117:358-364. 11. Chapman PD, Vetter JW, Souza JJ. et al. Gompara-
6, Winkle RA, Mead RH, Ruder MA, et al. Improved tive efficacy of monophasic and biphasic truncated
low energy defibrillation efficacy in man with the exponential shocks for nonthoracotomy internal
1410 July 1993. Part I PAGE, Vol. 16
EFFECT OF WAVESHAPE ON DEFIBRILLATION
defibrillation in dogs. J Am Coll Cardiol 1988; 12: 19. Koning G. Some physical aspects of ventricular de-
739-745. fibrillation: A system analytic approach. Amster-
12. Jones )L, [ones RE. Balasky G. Improved cardiac dam, The Netherlands, Free University of Amster-
cell excitation with symmetrical biphasic defibril- dam, 1972.
lator waveforms. Am J Physiol 1987; 253:H1418- 20. Rauglas E, Blazek Z, Vrana M. Efficacy of mono-
H1424. phasitj eiectricai impulses with steep leading and
13. Jone.s ]L. Jones RE. Improved safety factors for tri- trailing edges in cardiac defibrillation. Cor Vasa
phasic defibrillator waveforms. Circ Res 1989; 64: 1977: 19;37B-384.
1172-1177. 21. Daubert ]P, Frazier DW, Wolf PD. et al. Response
14. Swartz JF. Jones JL, Jones RE, et al. Conditioning of relatively refractory canine myocardium to mo-
prepulse of biphasic defibrillator waveforms en- nophasic and biphasic shocks. Girculation 1991;
hances refractoriness to fibrillation wavefronts. 84:2522-2538.
Circ Res 1991; 68:438-449. 22. Wbarton JM, Richard V), Murry CE Jr, et al. Electro-
15. Schuder JC, Rahmoeller GA. Stoeckle H. Transtho- physiologic effects in vivo of monophasic and bi-
racic ventricular defibrillation with triangular and phasic stimuli in normal and infarcted dogs. PACE
trapezoidal waveforms. Circ Res 1966; 19: 1990; 13:1158-1172.
689-694. 23. Zhou X, Knisley SB, Wolf PD, et al. Prolongation
16. National Research Council. Committee on the Care of repoiarization time by electric field stimulation
and Use of Laboratory Animals: United with monophasic and biphasic shocks in open
States—Revised 1985. Washington. DC, US Gov- chest dogs. Circ Res 1991; 68:1761-1767.
ernment Printing Office, 1985. 24. Wessale JL. Bipolar Catheter Defibrillation in Dogs
17. Angelakos ET, Torres JC. The efficiency of electri- Using Trapezoidal Waveforms of Various Tilts. W.
cal pulses for cardiac stimulation. Cardiologia Lafayette, IN, Purdue University. 1978.
1964; 44:355-365. 25. Tchou P, Krum D, Akhtar M, et al. Reduction of
18. Roy OZ, Wehnert RW. A more efficient waveform defibrillatiou energy requirements with a new bi-
for cardiac stimulation. Med Biol Eng 1971; 9; phasic waveform, (abstract) PACE 1990; 13:506.
495-501.
PACE, Vol. 16 July 1993, Part I 1411
Você também pode gostar
- Prader Willi SyndromeDocumento14 páginasPrader Willi Syndromeapi-471834071Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Home Care Catalogue UK Edition 4 Web PDFDocumento60 páginasHome Care Catalogue UK Edition 4 Web PDFmanuales tecnicosAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Dispelling Myths About Drinking Distilled WaterDocumento6 páginasDispelling Myths About Drinking Distilled WaterPau StraitAinda não há avaliações
- Choosing An Enteral Feeding FormulaDocumento44 páginasChoosing An Enteral Feeding FormulaMeta Hanindita NugrohoAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- IAF MD 8 2011 Application of ISO 17011 in MDQMS (ISO 13485) Issue 1 2011Documento17 páginasIAF MD 8 2011 Application of ISO 17011 in MDQMS (ISO 13485) Issue 1 2011carlosprieto36Ainda não há avaliações
- Can Coloring Mandalas Reduce AnxietyDocumento6 páginasCan Coloring Mandalas Reduce AnxietyAbirAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- OralMeds - ChecklistDocumento6 páginasOralMeds - ChecklistXandra BasnilloAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Updates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionDocumento12 páginasUpdates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionMarietta_MonariAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- TM ModuleDocumento57 páginasTM Moduleprincess lyn castromayorAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hydro CollatorDocumento24 páginasHydro CollatorSreeraj S R100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Kellian-Hunte hw410 Unit 9 - Assignment-Stress - Critical Issues in Management and PreventionDocumento8 páginasKellian-Hunte hw410 Unit 9 - Assignment-Stress - Critical Issues in Management and Preventionapi-616884609Ainda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Diseases of The Immune System: OBC 231 General PathologyDocumento91 páginasDiseases of The Immune System: OBC 231 General PathologyRana MohammadAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- 1760Documento11 páginas1760AnggunAinda não há avaliações
- Jurnal SkoliosisDocumento9 páginasJurnal SkoliosisLidya SiahaanAinda não há avaliações
- Introduction To Occupational TherapyDocumento50 páginasIntroduction To Occupational TherapyDevy CaruzAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Antibiotics ChartDocumento10 páginasAntibiotics Chartadom09Ainda não há avaliações
- Interferential Stimulation For The Treatment of Musculoskeletal PainDocumento15 páginasInterferential Stimulation For The Treatment of Musculoskeletal PainCTAFDocumentsAinda não há avaliações
- Play TherapyDocumento4 páginasPlay TherapyAnita Hani ChristinaAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- HRM Research PaperDocumento20 páginasHRM Research PaperJames Monsanto100% (1)
- FNB-Minimal Access Surgery: Competency Based Training ProgrammeDocumento31 páginasFNB-Minimal Access Surgery: Competency Based Training ProgrammeAMBUJ KUMAR SONIAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- BMR Revision TimelineDocumento33 páginasBMR Revision TimelineYihui WongAinda não há avaliações
- HandDocumento95 páginasHandAsad noor mirzaAinda não há avaliações
- Ways of Enhancing Pulp Preservation by Stepwise Excavation-A Systematic Review PDFDocumento13 páginasWays of Enhancing Pulp Preservation by Stepwise Excavation-A Systematic Review PDFFabian ArangoAinda não há avaliações
- Pregnancy: Signs/Symptoms and Common Health ConcernsDocumento5 páginasPregnancy: Signs/Symptoms and Common Health ConcernsTracy50% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Tina Dobbs Health Department ReportDocumento12 páginasTina Dobbs Health Department ReportAdamCareyAinda não há avaliações
- South West Regional Bulletin: A Message From The Director All Change at The CentreDocumento19 páginasSouth West Regional Bulletin: A Message From The Director All Change at The Centre433188Ainda não há avaliações
- Antenatal Diet PlanDocumento7 páginasAntenatal Diet PlanSunija Selvam100% (3)
- Cmagbanua Aicbm Handout 2s 127pDocumento127 páginasCmagbanua Aicbm Handout 2s 127pWilliam Tell100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Healthcare Hospital MaintenanceDocumento302 páginasHealthcare Hospital Maintenanceshahar397100% (2)
- Pharmaceutics IntroductionDocumento9 páginasPharmaceutics IntroductionVIJAY KUMAR TIRUKKACHIAinda não há avaliações