Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Oral Histology MCQ Quiz PDFDocumento77 páginasOral Histology MCQ Quiz PDFaaaa86% (7)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Frog Dissection Answer WorksheetDocumento7 páginasFrog Dissection Answer Worksheetapi-23318756633% (3)
- King Saud University Dental Residents' Continuing Education Course in Oral BiologyDocumento6 páginasKing Saud University Dental Residents' Continuing Education Course in Oral BiologyMuhamad Andika Arief PutranamiAinda não há avaliações
- 113B Selective Grinding ReviewDocumento19 páginas113B Selective Grinding ReviewPragati ParasherAinda não há avaliações
- Laboratary Lab ReportDocumento6 páginasLaboratary Lab ReportMaarveen RajAinda não há avaliações
- Pragyan College of Nursing-Bhopal BSC Nursing 1 Year Subject-Anatomy and Physiology Topic-Sense of Taste/TongueDocumento3 páginasPragyan College of Nursing-Bhopal BSC Nursing 1 Year Subject-Anatomy and Physiology Topic-Sense of Taste/TongueNeelofur Ibran AliAinda não há avaliações
- Triune Brain - WikipediaDocumento4 páginasTriune Brain - WikipediaWilhelm Richard WagnerAinda não há avaliações
- Blood Types Transfusion Tissue and Organ Transplantation NotesDocumento7 páginasBlood Types Transfusion Tissue and Organ Transplantation NotesRama JoshiAinda não há avaliações
- Chronopharmacology of AntyhipertensionDocumento32 páginasChronopharmacology of AntyhipertensionENDANGAinda não há avaliações
- Histology 18 Male Reproductive SystemDocumento49 páginasHistology 18 Male Reproductive SystemAbdul RahmanAinda não há avaliações
- Medical Examiner's Report On Daniel PrudeDocumento8 páginasMedical Examiner's Report On Daniel PrudePatrick Crozier100% (1)
- What Does The Endocrine System Do?Documento10 páginasWhat Does The Endocrine System Do?hadiqa azizAinda não há avaliações
- Digestive System by Dr. Tehreem FatimaDocumento9 páginasDigestive System by Dr. Tehreem FatimaTehreem FatimaAinda não há avaliações
- WL-ES700 Manual Preso en InglesDocumento10 páginasWL-ES700 Manual Preso en InglesVerónica Barría JerezAinda não há avaliações
- Tissue TableDocumento4 páginasTissue TableMarcie BooneAinda não há avaliações
- Diploma in Human Anatomy and PhysiologyDocumento2 páginasDiploma in Human Anatomy and PhysiologyNaveed SakiAinda não há avaliações
- Craniofacial Changes in Patients With Class III Malocclusion Treated With The Rampa SystemDocumento7 páginasCraniofacial Changes in Patients With Class III Malocclusion Treated With The Rampa Systemapi-192260741100% (1)
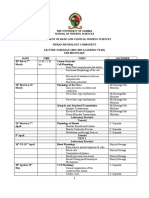
- Physiology Course OutlineDocumento4 páginasPhysiology Course OutlineSAVIOUR BANDAAinda não há avaliações
- Normoz TabletDocumento6 páginasNormoz TabletAmita VermaAinda não há avaliações
- Physiological Homeostasis ChapterDocumento16 páginasPhysiological Homeostasis ChapteraclumutAinda não há avaliações
- Acalculia - Clasificación, Etiología y Tratamiento ClínicoDocumento5 páginasAcalculia - Clasificación, Etiología y Tratamiento ClínicoNatalia Alarcón NavarroAinda não há avaliações
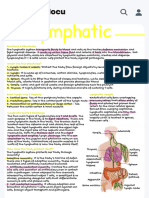
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocumento1 páginaHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieAinda não há avaliações
- Defense Mechanism of GingivaDocumento20 páginasDefense Mechanism of GingivaMuhammed MansoorAinda não há avaliações
- Skrining HK Pada GAKIDocumento33 páginasSkrining HK Pada GAKIdiyahAinda não há avaliações
- 2014 Helsinki Workshop Material ShacklockDocumento43 páginas2014 Helsinki Workshop Material ShacklockAl100% (1)
- How Exercise Improves the Cardiorespiratory SystemDocumento15 páginasHow Exercise Improves the Cardiorespiratory SystemBASAVARAJ100% (1)
- Tactile PathwayDocumento3 páginasTactile PathwayMae Angelie LabayaAinda não há avaliações
- Hema - Guide Notes PDFDocumento21 páginasHema - Guide Notes PDFVanessa Ladra100% (1)
- Impacted Teeth RemovalDocumento35 páginasImpacted Teeth RemovalChaitanya SuramAinda não há avaliações
- ANP105 Anatomy & PhysiologyDocumento29 páginasANP105 Anatomy & PhysiologyDayana Haziqa AkhbarAinda não há avaliações