Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Fetal Neurophysiology According To Gestational Age Aida Salihagic Kadic, Maja PredojevicDocumento5 páginasFetal Neurophysiology According To Gestational Age Aida Salihagic Kadic, Maja PredojevicDaniela Isidora San Martin CanalesAinda não há avaliações
- Intro To MycologyDocumento8 páginasIntro To Mycologycamille chuaAinda não há avaliações
- University of Limpopo School of Molecular and Life Sciences TestsDocumento10 páginasUniversity of Limpopo School of Molecular and Life Sciences TestsSjabuliso Madlala ThandekaAinda não há avaliações
- National Population PolicyDocumento6 páginasNational Population PolicychinchuAinda não há avaliações
- Sexuality in Older AdultDocumento10 páginasSexuality in Older AdultNisa100% (1)
- Supplemental Notes in Maternal Bullets Family PlanningDocumento3 páginasSupplemental Notes in Maternal Bullets Family Planningjohn paul richard mindanaoAinda não há avaliações
- Occult Forces of SexDocumento6 páginasOccult Forces of Seximmortality2045_841960% (5)
- Sissy Forum2Documento6 páginasSissy Forum2Ali NasirAinda não há avaliações
- Fraction of The Peripheral Blood Concentration of CD56 /CD16 /CD3 Cells in Total Natural Killer Cells As An Indication of Fertility and InfertilityDocumento7 páginasFraction of The Peripheral Blood Concentration of CD56 /CD16 /CD3 Cells in Total Natural Killer Cells As An Indication of Fertility and InfertilityqisthiaufaAinda não há avaliações
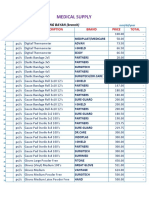
- Medical Supplies, & Baby Products PricelistDocumento5 páginasMedical Supplies, & Baby Products PricelistParmasya Ng Bayan Bacolor Main BranchAinda não há avaliações
- Starting Right With BeesDocumento27 páginasStarting Right With Beessezra1Ainda não há avaliações
- Copy-Induced Breeding in FishDocumento31 páginasCopy-Induced Breeding in Fishhafiz anasAinda não há avaliações
- Breast Cancer KelseyDocumento12 páginasBreast Cancer Kelseyapi-3802092Ainda não há avaliações
- Survey Tool Dummy TableDocumento10 páginasSurvey Tool Dummy TableJPJessiePaulAinda não há avaliações
- Artificial InseminationDocumento29 páginasArtificial InseminationMayuri VohraAinda não há avaliações
- Advantages of ContraceptivesDocumento4 páginasAdvantages of ContraceptivesArgel Linard Francisco MabagaAinda não há avaliações
- Does DHT Affect Transplanted HairDocumento2 páginasDoes DHT Affect Transplanted HairsahakhanshahAinda não há avaliações
- Artificial Insemination NotesDocumento3 páginasArtificial Insemination NotesMohsin DawarAinda não há avaliações
- Bicornuate Uterus With Associated Bilateral Tubal Blockage and Fibroid TumorsDocumento3 páginasBicornuate Uterus With Associated Bilateral Tubal Blockage and Fibroid TumorsPutu AndreAinda não há avaliações
- Handbook Pikeperch ReproductionDocumento80 páginasHandbook Pikeperch ReproductioniddiottAinda não há avaliações
- PC-PNDT ActDocumento34 páginasPC-PNDT ActDr. Rakshit SolankiAinda não há avaliações
- Uterine Hyperstimulation, Management of - ABMU Maternity Guideline 2018Documento7 páginasUterine Hyperstimulation, Management of - ABMU Maternity Guideline 2018Chintya MarcellinAinda não há avaliações
- Teen Pregnancy: Glorification Through Entertainment MediaDocumento5 páginasTeen Pregnancy: Glorification Through Entertainment MediaAshton TrumbleAinda não há avaliações
- Reproductive SystemDocumento56 páginasReproductive SystemRochelle Ann CunananAinda não há avaliações
- (TDS) SPL Ivf Culture DishDocumento2 páginas(TDS) SPL Ivf Culture DishRedouaneAinda não há avaliações
- Pi Is 001502821501924 XDocumento19 páginasPi Is 001502821501924 XahmadheulwanAinda não há avaliações
- Art Dynamic Morphology and Embryology PDFDocumento42 páginasArt Dynamic Morphology and Embryology PDFimageorge13Ainda não há avaliações
- Molecular Diagnostics-Fundamentals Methods and Clinical ApplicationsDocumento479 páginasMolecular Diagnostics-Fundamentals Methods and Clinical ApplicationsYasen Taha100% (9)
- The Role of Aspirin Dose On The Prevention of Preeclampsia and Fetal Growth Restriction: Systematic Review and Meta-AnalysisDocumento17 páginasThe Role of Aspirin Dose On The Prevention of Preeclampsia and Fetal Growth Restriction: Systematic Review and Meta-AnalysisfujimeisterAinda não há avaliações
- Newborn Essential Care PDFDocumento54 páginasNewborn Essential Care PDFMARK LENAND ESPIRITU100% (1)