Você também pode gostar
- 2013 14 International Student New ContractDocumento2 páginas2013 14 International Student New ContracthalovoaAinda não há avaliações
- Confidentiality and Non-Disclosure Agreement TemplateDocumento3 páginasConfidentiality and Non-Disclosure Agreement TemplateKALIDASS KAinda não há avaliações
- Ls - Confidentiality and Nondisclosure Agreement For ClientsDocumento2 páginasLs - Confidentiality and Nondisclosure Agreement For ClientsHeinz MilitarAinda não há avaliações
- Of Counsel Agreement FYIDocumento2 páginasOf Counsel Agreement FYIAnonymous v3dT7UF0% (1)
- Management Services AgreementDocumento9 páginasManagement Services AgreementLe Voeu0% (1)
- Copyright Infringement Cease and Desist LetterDocumento2 páginasCopyright Infringement Cease and Desist LetterLinda Ayu PertiwiAinda não há avaliações
- Vie TH Sales Rep AgreementDocumento4 páginasVie TH Sales Rep AgreementJohnAinda não há avaliações
- Cease and Desist Advance AutoDocumento2 páginasCease and Desist Advance AutoGersh KuntzmanAinda não há avaliações
- Negotiable InsturmentsDocumento19 páginasNegotiable Insturmentsishasingh14289Ainda não há avaliações
- Addendum To Contract of Sale (Chase) 12122011 WEB-1417029181Documento10 páginasAddendum To Contract of Sale (Chase) 12122011 WEB-1417029181Gleb SterrAinda não há avaliações
- SAMPLE Living WillDocumento2 páginasSAMPLE Living WillRichie HirschAinda não há avaliações
- Juneteenth Sponsorship Package 2015-2016fillableDocumento2 páginasJuneteenth Sponsorship Package 2015-2016fillableDenton JuneteenthAinda não há avaliações
- NdaDocumento1 páginaNdaounacersAinda não há avaliações
- Meg Letter of Intent - Hedge Road, PlymouthDocumento3 páginasMeg Letter of Intent - Hedge Road, PlymouthmegcostsusmillionsAinda não há avaliações
- Assignment and Transfer of Stock CertificateDocumento1 páginaAssignment and Transfer of Stock CertificateUlrichAinda não há avaliações
- Certifying A Document Policy - 2018Documento2 páginasCertifying A Document Policy - 2018kashansajjadAinda não há avaliações
- Ownership of CopyrightDocumento3 páginasOwnership of CopyrightMeghan Kaye LiwenAinda não há avaliações
- Mentorship 101Documento2 páginasMentorship 101Simon RobinsonAinda não há avaliações
- Repayment Agreement FormDocumento1 páginaRepayment Agreement FormbryanastollAinda não há avaliações
- Layer7 Referral AgreementV1Documento6 páginasLayer7 Referral AgreementV1george8406Ainda não há avaliações
- 047-1 Response Motion SanctionsDocumento19 páginas047-1 Response Motion SanctionsEzekiel KobinaAinda não há avaliações
- Promissory Note TemplateDocumento5 páginasPromissory Note TemplateJason AbanesAinda não há avaliações
- US Internal Revenue Service: f1041t - 1998Documento2 páginasUS Internal Revenue Service: f1041t - 1998IRSAinda não há avaliações
- Membership Interest Purchase AgreementDocumento7 páginasMembership Interest Purchase Agreementjth2698Ainda não há avaliações
- Fee ScheduleDocumento10 páginasFee ScheduleNorth DlsaAinda não há avaliações
- Copyright Assignment AgreementDocumento4 páginasCopyright Assignment AgreementGiyukichanAinda não há avaliações
- Payroll Services AgreementDocumento5 páginasPayroll Services AgreementAugustoAinda não há avaliações
- Artist Agent Agreement 2010-05-13Documento12 páginasArtist Agent Agreement 2010-05-13Patrick ChevrelAinda não há avaliações
- Release For Property Damage in Auto AccidentDocumento3 páginasRelease For Property Damage in Auto AccidentKent WhiteAinda não há avaliações
- Demand For BOPDocumento8 páginasDemand For BOPtitledanAinda não há avaliações
- Tennessee Living WillDocumento2 páginasTennessee Living WillRocketLawyer100% (1)
- NDA SampleDocumento5 páginasNDA SampleHein Sithu KyawAinda não há avaliações
- Trademark Assignment Service MarkassignDocumento8 páginasTrademark Assignment Service MarkassignCane Cirpo100% (1)
- Non-Disclosure AgreementDocumento4 páginasNon-Disclosure AgreementRegarian TaringAinda não há avaliações
- Gig ContractDocumento1 páginaGig ContractMichael KeplingerAinda não há avaliações
- Data Confidentiality TemplateDocumento6 páginasData Confidentiality Templatebjaguar33Ainda não há avaliações
- GTP-RPS Release and Settlement AgreementDocumento6 páginasGTP-RPS Release and Settlement AgreementinforumdocsAinda não há avaliações
- Sample Company Credit Card Usage PolicyDocumento4 páginasSample Company Credit Card Usage PolicyPremalAinda não há avaliações
- Independent Contractor AgreementDocumento6 páginasIndependent Contractor AgreementShaqqaAinda não há avaliações
- ComplaintDocumento75 páginasComplaintDaniel Taylor100% (1)
- Purchase AgreementDocumento3 páginasPurchase AgreementPedro Ant. Núñez UlloaAinda não há avaliações
- Quitclaim Deed: These Forms Are Not A Substitute For Legal Advice.Documento2 páginasQuitclaim Deed: These Forms Are Not A Substitute For Legal Advice.DellAinda não há avaliações
- NY Power of Attorney FormDocumento7 páginasNY Power of Attorney Formponticarlo76580% (1)
- 04/26/2013: Meeting of The Directors of The New York State Urban Development Corporation D/b/a Empire State Development (New York, NY) 9:30 A.M.Documento188 páginas04/26/2013: Meeting of The Directors of The New York State Urban Development Corporation D/b/a Empire State Development (New York, NY) 9:30 A.M.Empire State DevelopmentAinda não há avaliações
- Kyle Rowe NC PetitionDocumento4 páginasKyle Rowe NC PetitionjustinmcAinda não há avaliações
- RLTO Case LawDocumento11 páginasRLTO Case LawChicagoMTOAinda não há avaliações
- Participation AgreementDocumento6 páginasParticipation AgreementDanilo Magallanes Sampaga100% (1)
- Single Member LLC Operating AgreementDocumento7 páginasSingle Member LLC Operating AgreementRamon De LeonAinda não há avaliações
- Law Partnership Agreement With Provisions For The Death, Retirement, Withdrawal, or Expulsion of A PartnerDocumento2 páginasLaw Partnership Agreement With Provisions For The Death, Retirement, Withdrawal, or Expulsion of A PartnerKaya YurtkuranAinda não há avaliações
- Venue Use Agreement - RNC and RochesterDocumento4 páginasVenue Use Agreement - RNC and RochesterSean BakerAinda não há avaliações
- Non Circumvention Non Disclosure Agreement (TERENCE) SGDocumento7 páginasNon Circumvention Non Disclosure Agreement (TERENCE) SGLin ChrisAinda não há avaliações
- Mutual Termination of ContractDocumento1 páginaMutual Termination of ContractRose AsiamahAinda não há avaliações
- Return Policy: Step 1Documento2 páginasReturn Policy: Step 1Gamer BuddyAinda não há avaliações
- Sacramento Auto Accident AttorneyDocumento5 páginasSacramento Auto Accident AttorneyMona DeldarAinda não há avaliações
- First Discovery Request in Brown-Dickerson v. City of Philadelphia, Et AlDocumento6 páginasFirst Discovery Request in Brown-Dickerson v. City of Philadelphia, Et AlThe DeclarationAinda não há avaliações
- RE: Notice and Praccipe, Contract Termination: Enclosure - Driver's License Card NoDocumento2 páginasRE: Notice and Praccipe, Contract Termination: Enclosure - Driver's License Card NotomjoneshaslotstodoAinda não há avaliações
- Divorce in Connecticut: The Legal Process, Your Rights, and What to ExpectNo EverandDivorce in Connecticut: The Legal Process, Your Rights, and What to ExpectAinda não há avaliações
- Administrative Clerk: Passbooks Study GuideNo EverandAdministrative Clerk: Passbooks Study GuideAinda não há avaliações
- Civil Government of Virginia: A Text-book for Schools Based Upon the Constitution of 1902 and Conforming to the Laws Enacted in Accordance TherewithNo EverandCivil Government of Virginia: A Text-book for Schools Based Upon the Constitution of 1902 and Conforming to the Laws Enacted in Accordance TherewithAinda não há avaliações
- PERSONAL DEVELOPMENT (What Is Personal Development?)Documento37 páginasPERSONAL DEVELOPMENT (What Is Personal Development?)Ronafe Roncal GibaAinda não há avaliações
- Solution Documentation For Custom DevelopmentDocumento52 páginasSolution Documentation For Custom DevelopmentbayatalirezaAinda não há avaliações
- Reclaimer PDFDocumento8 páginasReclaimer PDFSiti NurhidayatiAinda não há avaliações
- Chapter 2.2 Quantitative Analysis NewDocumento44 páginasChapter 2.2 Quantitative Analysis NewMinase TilayeAinda não há avaliações
- Cable Schedule - Instrument - Surfin - Malanpur-R0Documento3 páginasCable Schedule - Instrument - Surfin - Malanpur-R0arunpandey1686Ainda não há avaliações
- Bleed Valve FunctionDocumento7 páginasBleed Valve FunctionUWT10Ainda não há avaliações
- Regression Week 2: Multiple Linear Regression Assignment 1: If You Are Using Graphlab CreateDocumento1 páginaRegression Week 2: Multiple Linear Regression Assignment 1: If You Are Using Graphlab CreateSamAinda não há avaliações
- History of JavaDocumento3 páginasHistory of JavaKyra ParaisoAinda não há avaliações
- Volvo HU 803Documento8 páginasVolvo HU 803GiegloAinda não há avaliações
- Cot Observation ToolDocumento14 páginasCot Observation ToolArnoldBaladjayAinda não há avaliações
- Building g5Documento45 páginasBuilding g5ammarsteel68Ainda não há avaliações
- Din 48204Documento3 páginasDin 48204Thanh Dang100% (4)
- Ems Speed Sensor Com MotorDocumento24 páginasEms Speed Sensor Com MotorKarina RickenAinda não há avaliações
- Lecture No. 11Documento15 páginasLecture No. 11Sayeda JabbinAinda não há avaliações
- Philippine Rural Development Project: South Luzon Cluster C Ommunication Resourc ES Management WorkshopDocumento45 páginasPhilippine Rural Development Project: South Luzon Cluster C Ommunication Resourc ES Management WorkshopAlorn CatibogAinda não há avaliações
- Assignment 1 - Vertical Alignment - SolutionsDocumento6 páginasAssignment 1 - Vertical Alignment - SolutionsArmando Ramirez100% (1)
- Modicon PLC CPUS Technical Details.Documento218 páginasModicon PLC CPUS Technical Details.TrbvmAinda não há avaliações
- RTD IncotestDocumento2 páginasRTD IncotestJabari KaneAinda não há avaliações
- Datasheet 6A8 FusívelDocumento3 páginasDatasheet 6A8 FusívelMluz LuzAinda não há avaliações
- BIM and Big Data For Construction Cost ManagementDocumento46 páginasBIM and Big Data For Construction Cost Managementlu09100% (1)
- Digital Speed Control of DC Motor For Industrial Automation Using Pulse Width Modulation TechniqueDocumento6 páginasDigital Speed Control of DC Motor For Industrial Automation Using Pulse Width Modulation TechniquevendiAinda não há avaliações
- CNNPX310R-6P: General SpecificationsDocumento5 páginasCNNPX310R-6P: General SpecificationsZoheir KacimiAinda não há avaliações
- Asugal Albi 4540Documento2 páginasAsugal Albi 4540dyetex100% (1)
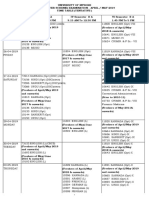
- Ugtt April May 2019 NewDocumento48 páginasUgtt April May 2019 NewSuhas SAinda não há avaliações
- Video Course NotesDocumento18 páginasVideo Course NotesSiyeon YeungAinda não há avaliações
- ModelsimDocumento47 páginasModelsimKishor KumarAinda não há avaliações
- End Points SubrogadosDocumento3 páginasEnd Points SubrogadosAgustina AndradeAinda não há avaliações
- Perbandingan Implementasi Smart City Di Indonesia: Studi Kasus: Perbandingan Smart People Di Kota Surabaya Dan Kota MalangDocumento11 páginasPerbandingan Implementasi Smart City Di Indonesia: Studi Kasus: Perbandingan Smart People Di Kota Surabaya Dan Kota Malanglely ersilyaAinda não há avaliações
- Day 2 - Evident's Official ComplaintDocumento18 páginasDay 2 - Evident's Official ComplaintChronicle Herald100% (1)
- Starex Is BTSDocumento24 páginasStarex Is BTSKLAinda não há avaliações