Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
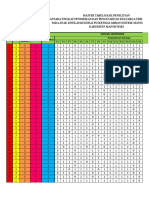
- Lampiran 4: NO Karakteristik Responden Variabel Independen Umur Pekerjaan Pendidikan Pengetahuan Keluarga Jenis KelaminDocumento4 páginasLampiran 4: NO Karakteristik Responden Variabel Independen Umur Pekerjaan Pendidikan Pengetahuan Keluarga Jenis KelaminFahriAinda não há avaliações
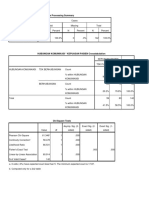
- Case Processing SummaryDocumento2 páginasCase Processing SummaryFahriAinda não há avaliações
- Colloid Surface Chemistry Critically Affects Multiple Particle Tracking Measurements of BiomaterialsDocumento11 páginasColloid Surface Chemistry Critically Affects Multiple Particle Tracking Measurements of BiomaterialsFahriAinda não há avaliações
- Universal Diffusion-Limited Colloid Aggregation: H DA R RC P TDocumento22 páginasUniversal Diffusion-Limited Colloid Aggregation: H DA R RC P TFahriAinda não há avaliações
- Melhus Et Al-1999-Journal of Bone and Mineral Research PDFDocumento7 páginasMelhus Et Al-1999-Journal of Bone and Mineral Research PDFFahriAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- 9 0 Development and OperatingDocumento12 páginas9 0 Development and OperatingAnu Partha100% (1)
- An Isogeometric Analysis Approach For The Study of Structural VibrationsDocumento59 páginasAn Isogeometric Analysis Approach For The Study of Structural VibrationsBharti SinghAinda não há avaliações
- Flue Gas Analysis in IndustryDocumento150 páginasFlue Gas Analysis in Industryblack_knight728Ainda não há avaliações
- Fire InvestigationDocumento126 páginasFire InvestigationAbcede IloiloAinda não há avaliações
- Assignment 176020307045 PDFDocumento82 páginasAssignment 176020307045 PDFnikita gohelAinda não há avaliações
- Electronic Modular Control Panel II Paralleling Emcp II P Systems Operation Troubleshooting Testing and Adjusting CaterpillarDocumento200 páginasElectronic Modular Control Panel II Paralleling Emcp II P Systems Operation Troubleshooting Testing and Adjusting CaterpillarAbdo MalkiAinda não há avaliações
- WJMDocumento6 páginasWJMAldianivo Nur FaizAinda não há avaliações
- Dual Axis Solar Activity Tracker For Solar Panels: Department of Engineering, Sciences and Humanities (DESH)Documento5 páginasDual Axis Solar Activity Tracker For Solar Panels: Department of Engineering, Sciences and Humanities (DESH)sujay patilAinda não há avaliações
- 1 - Classful Ip AddressingDocumento6 páginas1 - Classful Ip AddressingBiruk Tesfaye Legesse100% (1)
- The Mathematical Society of Serbia - 60 YearsDocumento23 páginasThe Mathematical Society of Serbia - 60 YearsBranko Ma Branko TadicAinda não há avaliações
- DefaultDocumento49 páginasDefaultmaruka33100% (1)
- IIEE La Union Harmonics AnalysisDocumento128 páginasIIEE La Union Harmonics AnalysisCarlnagum 123456789Ainda não há avaliações
- Rsa Netwitness Logs and Packets: Server, Dac and San HW SpecificationsDocumento10 páginasRsa Netwitness Logs and Packets: Server, Dac and San HW SpecificationsfunyiroemberAinda não há avaliações
- BIBLIOMETRICDocumento30 páginasBIBLIOMETRICkalaranishanmuganathAinda não há avaliações
- Understanding The Use of Ofdm in Ieee 802.16 (Wimax) : Roberto SacchiDocumento8 páginasUnderstanding The Use of Ofdm in Ieee 802.16 (Wimax) : Roberto SacchiHarald KerresAinda não há avaliações
- Digital - 123328-R010818-Analisa Balik-BibliografiDocumento5 páginasDigital - 123328-R010818-Analisa Balik-BibliografiEncep Septian CaturAinda não há avaliações
- Traulsen RLT - ALT Freezer DUTDocumento2 páginasTraulsen RLT - ALT Freezer DUTwsfc-ebayAinda não há avaliações
- Earthquake EnginneringDocumento11 páginasEarthquake EnginneringkkkAinda não há avaliações
- JAVA NotesDocumento12 páginasJAVA NotesVarun BawaAinda não há avaliações
- Analytic Geometry Parabola ProblemsDocumento14 páginasAnalytic Geometry Parabola ProblemsOjit QuizonAinda não há avaliações
- Ar 4201 PDFDocumento22 páginasAr 4201 PDFRiyanPratomuSiregarAinda não há avaliações
- Chapter 3 Ni ChupaghettiDocumento2 páginasChapter 3 Ni ChupaghettiRodemar RosarioAinda não há avaliações
- AMC Measurement ProblemsDocumento2 páginasAMC Measurement ProblemseltoAinda não há avaliações
- AC Induction Motors - How AC Motors WorkDocumento10 páginasAC Induction Motors - How AC Motors WorkBraulio IrrutiaAinda não há avaliações
- Hemoglobin A1c: A) MES 2-Morpholinoethane Sulfonic Acid B) TRIS Tris (Hydroxymethyl) - AminomethaneDocumento6 páginasHemoglobin A1c: A) MES 2-Morpholinoethane Sulfonic Acid B) TRIS Tris (Hydroxymethyl) - Aminomethanejoudi.jou95Ainda não há avaliações
- Postmodernity in PiDocumento2 páginasPostmodernity in Pixhardy27Ainda não há avaliações
- HCS2000Documento6 páginasHCS2000Nermin PalićAinda não há avaliações
- Sensor Gaurd Installation and Maintenance ManualDocumento57 páginasSensor Gaurd Installation and Maintenance ManualCapacitacion TodocatAinda não há avaliações
- 1 Egg & Egg Cookery LectureDocumento15 páginas1 Egg & Egg Cookery LectureErin DelavinAinda não há avaliações
- Simple MachinesDocumento25 páginasSimple MachinesMay ArispeAinda não há avaliações