Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Arthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDFDocumento569 páginasArthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDF'Minerva AlejandraAinda não há avaliações
- Do The Anterior and Lateral Thalamic Nuclei Make Distinct Contributions?Documento10 páginasDo The Anterior and Lateral Thalamic Nuclei Make Distinct Contributions?'Minerva AlejandraAinda não há avaliações
- Transcranial Electric Stimulation For The Investigation of Speech PerceptionDocumento14 páginasTranscranial Electric Stimulation For The Investigation of Speech Perception'Minerva AlejandraAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
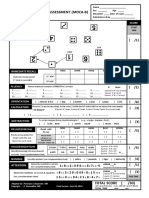
- MOCA Basic PDFDocumento2 páginasMOCA Basic PDF'Minerva AlejandraAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- 2015 Grieco Down Syndrome LifespanDocumento15 páginas2015 Grieco Down Syndrome Lifespan'Minerva AlejandraAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Cognición SocialDocumento10 páginasCognición Social'Minerva AlejandraAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Diabetic Foot Ulcers and Their RecurrenceDocumento9 páginasDiabetic Foot Ulcers and Their RecurrenceRoberto López MataAinda não há avaliações
- DCL ReversibleDocumento8 páginasDCL Reversible'Minerva AlejandraAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Bibliotecas MedicinaDocumento1 páginaBibliotecas Medicina'Minerva AlejandraAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Mecanism of AttentionDocumento21 páginasMecanism of Attention'Minerva AlejandraAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Daily Lesson LogDocumento4 páginasDaily Lesson LogPhebe Zhie Zhia CampeñaAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Fat Best Practices Guidelines PDFDocumento2 páginasFat Best Practices Guidelines PDFRosa VelásquezAinda não há avaliações
- Poststructuralism: Post-Structuralism Means After Structuralism. However, The Term Also Strongly ImpliesDocumento5 páginasPoststructuralism: Post-Structuralism Means After Structuralism. However, The Term Also Strongly ImpliesjuckballeAinda não há avaliações
- Wcdma Optimization GuideDocumento2 páginasWcdma Optimization GuideBenaiad AbdellahAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Civil Engineering 2018 2019Documento9 páginasCivil Engineering 2018 2019TbyTanAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Short CV: Prof. Dr. Zulkardi, M.I.Komp., MSCDocumento39 páginasShort CV: Prof. Dr. Zulkardi, M.I.Komp., MSCDika Dani SeptiatiAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- NetflixDocumento18 páginasNetflixLei Yunice NorberteAinda não há avaliações
- Form 2 MathematicsDocumento9 páginasForm 2 MathematicstarbeecatAinda não há avaliações
- Priya Gupta - Expansion and Electron Temperature Evolution in An Ultracold Neutral PlasmaDocumento184 páginasPriya Gupta - Expansion and Electron Temperature Evolution in An Ultracold Neutral PlasmaItama23Ainda não há avaliações
- MB700.4 Managerial Economics Quiz 1 MarksDocumento3 páginasMB700.4 Managerial Economics Quiz 1 MarksJAY SolankiAinda não há avaliações
- Creating A Cost Conscious Culture - CountingCostsDocumento20 páginasCreating A Cost Conscious Culture - CountingCostsRamona LutchmeesinghAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Unidad 2 InglesDocumento6 páginasUnidad 2 InglesAnonymous xt0Z7taDAinda não há avaliações
- Catrina Villalpando ResumeDocumento1 páginaCatrina Villalpando Resumeapi-490106460Ainda não há avaliações
- 1.1 Physical Qualtities CIE IAL Physics MS Theory UnlockedDocumento6 páginas1.1 Physical Qualtities CIE IAL Physics MS Theory Unlockedmaze.putumaAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- F240 Early Childhood Education Inners FINAL Web PDFDocumento319 páginasF240 Early Childhood Education Inners FINAL Web PDFSandra ClAinda não há avaliações
- Unit 2: TUTOR S NAME: - SCHEDULE: SÁB 7-12Documento4 páginasUnit 2: TUTOR S NAME: - SCHEDULE: SÁB 7-12Maria RadaAinda não há avaliações
- Social Work Practice and Social Welfare Policy in The United States A History (Philip R. Popple)Documento393 páginasSocial Work Practice and Social Welfare Policy in The United States A History (Philip R. Popple)5819Elis RahmawatiAinda não há avaliações
- Indian Institute of Forest ManagmentDocumento10 páginasIndian Institute of Forest ManagmentLabeeb HRtzAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- JAVIER KMeans Clustering Jupyter NotebookDocumento7 páginasJAVIER KMeans Clustering Jupyter NotebookAlleah LayloAinda não há avaliações
- Activity 4 Written Assessment - BambaDocumento3 páginasActivity 4 Written Assessment - BambaMatsuoka LykaAinda não há avaliações
- Projects and Programmes Committee ReportDocumento5 páginasProjects and Programmes Committee ReportElbekriAinda não há avaliações
- Tle Housekeeping 1st Module 5-Prepare Rooms For Guests (RG) Make Up Beds (For Teacher)Documento21 páginasTle Housekeeping 1st Module 5-Prepare Rooms For Guests (RG) Make Up Beds (For Teacher)Kate Cornelio100% (1)
- (2019) Piecewise Reproducing Kernel Method For Linear Impulsive Delay Differential Equations With Piecewise Constant ArgumentsDocumento10 páginas(2019) Piecewise Reproducing Kernel Method For Linear Impulsive Delay Differential Equations With Piecewise Constant ArgumentsAlejandro ChiuAinda não há avaliações
- Lesson Plan English Year 5Documento8 páginasLesson Plan English Year 5NurAiniNasirAinda não há avaliações
- Professional Nursing ResumeDocumento5 páginasProfessional Nursing Resumeapi-556406464Ainda não há avaliações
- Google Cloud Sales Credential 1Documento7 páginasGoogle Cloud Sales Credential 1Gaurav Nanda100% (1)
- A Level Design and Technology CourseworkDocumento5 páginasA Level Design and Technology Courseworkf6a3pzjr100% (2)
- Curriculum Vitae - Updated May 2020Documento6 páginasCurriculum Vitae - Updated May 2020api-513020529Ainda não há avaliações
- What Are The Six Dimensions of HealthDocumento5 páginasWhat Are The Six Dimensions of Healthqwerty hulaan moAinda não há avaliações
- Total Assessment Guide: Psychology Ch. 1Documento34 páginasTotal Assessment Guide: Psychology Ch. 1TruettCoffieldAinda não há avaliações