Você também pode gostar
- 2016 Article 229Documento7 páginas2016 Article 229nisa_kartikaAinda não há avaliações
- Accepted Manuscript: 10.1016/j.ajo.2014.05.016Documento20 páginasAccepted Manuscript: 10.1016/j.ajo.2014.05.016Anonymous iInKGkMCAinda não há avaliações
- Visualization and Grading of Vitreous Floaters Using Dynamic Ultra-Widefield Infrared Confocal Scanning Laser Ophthalmoscopy A Pilot StudyDocumento15 páginasVisualization and Grading of Vitreous Floaters Using Dynamic Ultra-Widefield Infrared Confocal Scanning Laser Ophthalmoscopy A Pilot Studymistic0Ainda não há avaliações
- Outcomes of Deep Sclerectomy Following Failed XENDocumento13 páginasOutcomes of Deep Sclerectomy Following Failed XENSagar ShahAinda não há avaliações
- Comparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesDocumento7 páginasComparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesVlady BordaAinda não há avaliações
- Clinical Utility of Optical Coherence Tomography in GlaucomaDocumento12 páginasClinical Utility of Optical Coherence Tomography in GlaucomaOkta Kurniawan SaputraAinda não há avaliações
- s12886 022 02600 XDocumento8 páginass12886 022 02600 XHariom ShuklaAinda não há avaliações
- RiboflavinUltravioletAinduced Collagen Wollensak Et Al Keratoconus 2003Documento8 páginasRiboflavinUltravioletAinduced Collagen Wollensak Et Al Keratoconus 2003SergioAinda não há avaliações
- Clinical Study of Intraocular Pressure Changesfollowing Nd-Yag Laser Iridotomy in Angle Closure DiseaseDocumento15 páginasClinical Study of Intraocular Pressure Changesfollowing Nd-Yag Laser Iridotomy in Angle Closure DiseaseIJAR JOURNALAinda não há avaliações
- MIGSDocumento12 páginasMIGSSyeda F AmbreenAinda não há avaliações
- Ajphe v3 Id1036Documento4 páginasAjphe v3 Id1036Amirah PaneAinda não há avaliações
- Focal Structure-Function Relationships in Primary Open-Angle Glaucoma Using OCT and OCT-A MeasurementsDocumento10 páginasFocal Structure-Function Relationships in Primary Open-Angle Glaucoma Using OCT and OCT-A MeasurementsAlejandro LondoñoAinda não há avaliações
- Seibold. Endoscopic CyclophotocoagulationDocumento12 páginasSeibold. Endoscopic CyclophotocoagulationJavier Infantes MolinaAinda não há avaliações
- OCT+Risley PrismDocumento3 páginasOCT+Risley PrismTony HajjAinda não há avaliações
- Wa0000Documento7 páginasWa0000Ocha24 TupamahuAinda não há avaliações
- Five-year results of viscotrabeculotomy vs conventional trabeculotomyDocumento10 páginasFive-year results of viscotrabeculotomy vs conventional trabeculotomyChintya Redina HapsariAinda não há avaliações
- Vitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyDocumento8 páginasVitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyVlady BordaAinda não há avaliações
- Pars Plana VitrekDocumento8 páginasPars Plana VitrekAnggisari Danastri DharmaAinda não há avaliações
- The Effectiveness of Laser Vitreolysis For Vitreous Floaters in Posterior Vitreous DetachmentDocumento7 páginasThe Effectiveness of Laser Vitreolysis For Vitreous Floaters in Posterior Vitreous Detachmentmistic0Ainda não há avaliações
- Cataract Surgery in Patients With Corneal Opacities: Researcharticle Open AccessDocumento10 páginasCataract Surgery in Patients With Corneal Opacities: Researcharticle Open AccesszulmiyettyAinda não há avaliações
- The Role of Widefield and Ultra Widefield Optical Coherence Tomography in The Diagnosis and Management of Vitreoretinal DiseasesDocumento17 páginasThe Role of Widefield and Ultra Widefield Optical Coherence Tomography in The Diagnosis and Management of Vitreoretinal Diseasesmistic0Ainda não há avaliações
- Keywords:-Tonometers, Intraocular Pressure, CentralDocumento6 páginasKeywords:-Tonometers, Intraocular Pressure, CentralInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Ascrs 2Documento7 páginasAscrs 2leokapilAinda não há avaliações
- 1 s2.0 S2451993620301249 MainDocumento4 páginas1 s2.0 S2451993620301249 MainHamidatun AnisaAinda não há avaliações
- Jurnal 1Documento6 páginasJurnal 1Gusti Tanjung Putera RahayuAinda não há avaliações
- Ophthalmology: Journal of and Advance ResearchDocumento14 páginasOphthalmology: Journal of and Advance ResearchAthenaeum Scientific PublishersAinda não há avaliações
- Trabeculectomy With Mitomycin-C in Post-Traumatic Angle Recession Glaucoma in Phakic Eyes With No Prior Intraocular InterventionDocumento7 páginasTrabeculectomy With Mitomycin-C in Post-Traumatic Angle Recession Glaucoma in Phakic Eyes With No Prior Intraocular InterventionJennifer ChavezAinda não há avaliações
- Current ConceptsDocumento300 páginasCurrent ConceptsGuilherme Bender LimaAinda não há avaliações
- Axial Myopia Is Associated With Visual Field Prognosis of Primary Open-Angle GlaucomaDocumento10 páginasAxial Myopia Is Associated With Visual Field Prognosis of Primary Open-Angle GlaucomaRezha IndrawanAinda não há avaliações
- Macular and Visual Outcomes After Cataract Extraction For Highly Myopic FoveoschisisDocumento5 páginasMacular and Visual Outcomes After Cataract Extraction For Highly Myopic Foveoschisisloshaana105Ainda não há avaliações
- The Effect of Trabeculectomy On Astigmatism .99150Documento5 páginasThe Effect of Trabeculectomy On Astigmatism .99150Yulias YoweiAinda não há avaliações
- Atlas OCT Angio in Diabetic Maculopathy Coscas enDocumento152 páginasAtlas OCT Angio in Diabetic Maculopathy Coscas enAlexandra FilipAinda não há avaliações
- Journal Reading - Dr. Sri Rejeki SinagaDocumento10 páginasJournal Reading - Dr. Sri Rejeki Sinagaamka chanAinda não há avaliações
- Journal Reading - Dr. Sri Rejeki SinagaDocumento10 páginasJournal Reading - Dr. Sri Rejeki Sinagaamka chanAinda não há avaliações
- Research ArticleDocumento9 páginasResearch ArticleRaissaAinda não há avaliações
- Vitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyDocumento9 páginasVitrectomy Combined With Posterior-Segment Ahmed Valve Implant: A Case Series StudyVlady BordaAinda não há avaliações
- A Practical Guide To Optical Coherence Tomography Angiography InterpretationDocumento17 páginasA Practical Guide To Optical Coherence Tomography Angiography InterpretationANIEAinda não há avaliações
- OJOph 2016062717483031Documento8 páginasOJOph 2016062717483031dechastraAinda não há avaliações
- BR J Ophthalmol-2014-Chan-79-81 PDFDocumento4 páginasBR J Ophthalmol-2014-Chan-79-81 PDFRomi Mauliza FauziAinda não há avaliações
- Jrs0215garzon 2Documento9 páginasJrs0215garzon 2Enrique Ferrando BarbenaAinda não há avaliações
- Segmentation Errors in Macular Ganglion Cell Analysis As Determined by Optical Coherence Tomography in Eyes With Macular PathologyDocumento8 páginasSegmentation Errors in Macular Ganglion Cell Analysis As Determined by Optical Coherence Tomography in Eyes With Macular PathologyMadhu C KAinda não há avaliações
- s12886 017 0419 1Documento8 páginass12886 017 0419 1Madhu C KAinda não há avaliações
- Sulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryDocumento6 páginasSulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryPrizilia SaimimaAinda não há avaliações
- Ijss Jun Oa14Documento4 páginasIjss Jun Oa14Yunanda RizkiAinda não há avaliações
- Ijss Jun Oa14Documento4 páginasIjss Jun Oa14Yunanda RizkiAinda não há avaliações
- Clinical Study: Two-Year Accelerated Corneal Cross-Linking Outcome in Patients With Progressive KeratoconusDocumento10 páginasClinical Study: Two-Year Accelerated Corneal Cross-Linking Outcome in Patients With Progressive KeratoconusPunam RazputriAinda não há avaliações
- Optical Coherence Tomography Angiography in Diabetic Retinopathy: An Updated ReviewDocumento13 páginasOptical Coherence Tomography Angiography in Diabetic Retinopathy: An Updated ReviewConnie STAinda não há avaliações
- Single-Step Transepithelial PHDocumento9 páginasSingle-Step Transepithelial PHlenniAinda não há avaliações
- Jurnal Mata 5Documento6 páginasJurnal Mata 5Dahru KinanggaAinda não há avaliações
- Therapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismDocumento7 páginasTherapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismStephanie PfengAinda não há avaliações
- Visual Acuity Outcome After Cataract SurgeryDocumento10 páginasVisual Acuity Outcome After Cataract SurgeryAi AisyahAinda não há avaliações
- Visual Outcomes of Diffractive Trifocal vs Monofocal IOLsDocumento11 páginasVisual Outcomes of Diffractive Trifocal vs Monofocal IOLsakun kd876Ainda não há avaliações
- 69 EdDocumento10 páginas69 EdAnna ListianaAinda não há avaliações
- Clinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsDocumento6 páginasClinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsAldoAinda não há avaliações
- 456 FullDocumento4 páginas456 FullYanjinlkham KhAinda não há avaliações
- The Effects of Laser Displacement On Femtosecond Laser-Assisted Conjunctival Autograft Preparation For Pterygium SurgeryDocumento15 páginasThe Effects of Laser Displacement On Femtosecond Laser-Assisted Conjunctival Autograft Preparation For Pterygium SurgerySavitri IndrasariAinda não há avaliações
- Clinical StudyDocumento6 páginasClinical StudyKarina Mega WAinda não há avaliações
- Resume 15Documento9 páginasResume 15Dyah PurwitaAinda não há avaliações
- Automated Direct Selective Laser Trabeculoplasty - First Prospective Clinical TrialDocumento11 páginasAutomated Direct Selective Laser Trabeculoplasty - First Prospective Clinical TrialMasha DiBAinda não há avaliações
- Zygomatic Implants: Optimization and InnovationNo EverandZygomatic Implants: Optimization and InnovationJames ChowAinda não há avaliações
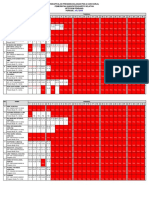
- Rekapitulasi Presensi Bulanan Pns (6 Hari Kerja) Pemerintah Kabupaten Barito Selatan Uptd PKM Pendang PeriodeDocumento3 páginasRekapitulasi Presensi Bulanan Pns (6 Hari Kerja) Pemerintah Kabupaten Barito Selatan Uptd PKM Pendang PeriodeFuad HadinataAinda não há avaliações
- Surat Edaran Idul Adha 2020Documento3 páginasSurat Edaran Idul Adha 2020Fuad HadinataAinda não há avaliações
- Jurnal Analisa Katarak FUAD CIS YENNYDocumento7 páginasJurnal Analisa Katarak FUAD CIS YENNYFuad HadinataAinda não há avaliações
- Jurnal Bahasa Ingrris Fuad HadinataDocumento3 páginasJurnal Bahasa Ingrris Fuad HadinataFuad HadinataAinda não há avaliações
- Jurnal Analisa Katarak FUAD CIS YENNYDocumento7 páginasJurnal Analisa Katarak FUAD CIS YENNYFuad HadinataAinda não há avaliações
- Jurnal Bahasa Ingrris Fuad HadinataDocumento3 páginasJurnal Bahasa Ingrris Fuad HadinataFuad HadinataAinda não há avaliações
- Daftar PustakaDocumento8 páginasDaftar PustakaStefan SaerangAinda não há avaliações
- Meridian Merilas 810 BrochureDocumento18 páginasMeridian Merilas 810 BrochureHaag-Streit UK (HS-UK)Ainda não há avaliações
- Aravind FAQs in Ophthalmology - 1 PDFDocumento708 páginasAravind FAQs in Ophthalmology - 1 PDFMilthon Catacora ContrerasAinda não há avaliações
- Dominance Wave Propagation During Binocular Rivalry in Mil - 2019 - Vision ReseaDocumento8 páginasDominance Wave Propagation During Binocular Rivalry in Mil - 2019 - Vision ReseaAaryan R SinghAinda não há avaliações
- Batch 31 P2S2 MCQ 2Documento21 páginasBatch 31 P2S2 MCQ 2Afiqi FikriAinda não há avaliações
- The Aging EyeDocumento53 páginasThe Aging EyeSenthil Kumar50% (2)
- Canadian Fellowship Directory April2018Documento30 páginasCanadian Fellowship Directory April2018Raúl Plasencia SaliniAinda não há avaliações
- Soal To Unand Unsri Usu Ix: Poin Total Isilah Pertanyaan Di Bawah Ini Dengan BenarDocumento21 páginasSoal To Unand Unsri Usu Ix: Poin Total Isilah Pertanyaan Di Bawah Ini Dengan BenarIbnu Gilang Syawali100% (1)
- The Side Effects of Corticosteroids: Bernard BeckerDocumento6 páginasThe Side Effects of Corticosteroids: Bernard BeckerShayyy JacksonAinda não há avaliações
- Blunt Trauma Management of EyeDocumento30 páginasBlunt Trauma Management of EyeeyepageAinda não há avaliações
- Aravind Eye Hospital Madurai: Apex Manual-2016Documento60 páginasAravind Eye Hospital Madurai: Apex Manual-2016umesh100% (3)
- Eye and Vision 7th EditionDocumento35 páginasEye and Vision 7th EditionCrystal LynaeAinda não há avaliações
- Lucas vs. Tuaño PDFDocumento23 páginasLucas vs. Tuaño PDFAnonymousAinda não há avaliações
- Nutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFDocumento64 páginasNutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFjvprasad100% (1)
- Dr. Liesa Zulhidya, SP.M: GlaucomaDocumento37 páginasDr. Liesa Zulhidya, SP.M: GlaucomaShapira alAinda não há avaliações
- Ocular Pharmacology - DR Fermin (2023)Documento5 páginasOcular Pharmacology - DR Fermin (2023)Patricia ManaliliAinda não há avaliações
- Questionnaire Survey Bases Awareness and Knowledge of Glaucoma Among Adult Patient in Rural and Urban Area in RaipurDocumento3 páginasQuestionnaire Survey Bases Awareness and Knowledge of Glaucoma Among Adult Patient in Rural and Urban Area in RaipurInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Visual Fields Interpretation in Glaucoma A Focus On Static Automated PerimetryDocumento8 páginasVisual Fields Interpretation in Glaucoma A Focus On Static Automated PerimetryMoisés Sergio Nina BaldeónAinda não há avaliações
- gt0912 F4 LarocheDocumento3 páginasgt0912 F4 LarocheMichael CraneAinda não há avaliações
- Jogi. Mcqs-1Documento47 páginasJogi. Mcqs-1Fazan Gem100% (3)
- IOA Scientific Meeting 2015 ScheduleDocumento252 páginasIOA Scientific Meeting 2015 ScheduleandarunfAinda não há avaliações
- 2007 SSS - AnswerDocumento7 páginas2007 SSS - AnswerResmin SihotangAinda não há avaliações
- Commonly Used Ophthalmic AbbreviationsDocumento2 páginasCommonly Used Ophthalmic Abbreviationshernan silvaAinda não há avaliações
- Try Out - UNSRIDocumento42 páginasTry Out - UNSRIekaAinda não há avaliações
- Atlas of Cataract SurgeryDocumento196 páginasAtlas of Cataract SurgeryDaniel Fernández Gajardo100% (3)
- Disorders of Special Senses 2020Documento68 páginasDisorders of Special Senses 2020Cres Padua Quinzon100% (1)
- Preperimetric GlaucomaDocumento65 páginasPreperimetric Glaucomaneha midhaAinda não há avaliações
- PCG Diagnosis & TreatmentDocumento15 páginasPCG Diagnosis & TreatmentPrashantha VespanathanAinda não há avaliações
- Zeiss SLT Broschuere en OUS - 31 - 011 - 0019IIDocumento5 páginasZeiss SLT Broschuere en OUS - 31 - 011 - 0019IIIrving AmadorAinda não há avaliações
- Eye MCQDocumento1 páginaEye MCQLoveKumarAinda não há avaliações