Você também pode gostar
- Current Chlamydia Trachomatis Infection, A Major Cause of InfertilityDocumento7 páginasCurrent Chlamydia Trachomatis Infection, A Major Cause of InfertilityRiany Jade SabrinaAinda não há avaliações
- Articulo 2 - El Microbiota Vaginal Se Asocia Con La Regresión de Neoplasia Intraepitelial CervicalDocumento13 páginasArticulo 2 - El Microbiota Vaginal Se Asocia Con La Regresión de Neoplasia Intraepitelial CervicalLiliana Antonio RevueltaAinda não há avaliações
- Composition of Vaginal Microbiota and Their Antibiotic Susceptibility in Symptomatic WomenDocumento6 páginasComposition of Vaginal Microbiota and Their Antibiotic Susceptibility in Symptomatic WomenAmirah MohdAinda não há avaliações
- Effects of Chlamydia Trachomatis Infection On Fertility A Case-Control StudyDocumento6 páginasEffects of Chlamydia Trachomatis Infection On Fertility A Case-Control StudyNoten80002 N8000Ainda não há avaliações
- Ijmmtd 24 171-174Documento5 páginasIjmmtd 24 171-174prabaAinda não há avaliações
- Dr. Vona 12Documento5 páginasDr. Vona 12Agustiawan ImronAinda não há avaliações
- Community Acquired Pneumonia In+childrenDocumento4 páginasCommunity Acquired Pneumonia In+childrendai shujuanAinda não há avaliações
- Hospital Management: Bacterial InfectionDocumento21 páginasHospital Management: Bacterial Infectionapadanainst7372Ainda não há avaliações
- Jurnal BVDocumento3 páginasJurnal BVEnvhy WinaAinda não há avaliações
- Association of High-Risk Cervical Human Papillomavirus With Demographic and Clinico - Pathological Features in Asymptomatic and Symptomatic WomenDocumento4 páginasAssociation of High-Risk Cervical Human Papillomavirus With Demographic and Clinico - Pathological Features in Asymptomatic and Symptomatic WomenInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Telaah Jurnal Annisa Nabilla 11120222180Documento20 páginasTelaah Jurnal Annisa Nabilla 11120222180annisa nabilaAinda não há avaliações
- Ref 5 PDFDocumento6 páginasRef 5 PDFGabriyah HamzahAinda não há avaliações
- Bacteriological Profile of Neonatal Sepsis and Antibiotic Susceptibility Pattern of Isolates Admitted at Kanti Children's Hospital, Kathmandu, NepalDocumento6 páginasBacteriological Profile of Neonatal Sepsis and Antibiotic Susceptibility Pattern of Isolates Admitted at Kanti Children's Hospital, Kathmandu, NepalPSIK sarimuliaAinda não há avaliações
- Retrospective Analysis of Prevalence of High-Risk and Low-Risk Human Papillomavirus (HPV) Genotypes in Iranian Women During 2013-2016Documento6 páginasRetrospective Analysis of Prevalence of High-Risk and Low-Risk Human Papillomavirus (HPV) Genotypes in Iranian Women During 2013-2016ruthcindy46Ainda não há avaliações
- 407 PDFDocumento4 páginas407 PDFSrideviRaviAinda não há avaliações
- 503 PDFDocumento5 páginas503 PDFAlda CarlyneAinda não há avaliações
- 6 Original CandiduriaDocumento7 páginas6 Original CandiduriaHarnadi WonogiriAinda não há avaliações
- Jurnal VaginalisDocumento6 páginasJurnal Vaginaliselsa prima putriAinda não há avaliações
- Effects of Chlamydia Trachomatis Infection On Fertility A Case-Control StudyDocumento7 páginasEffects of Chlamydia Trachomatis Infection On Fertility A Case-Control StudyRiany Jade SabrinaAinda não há avaliações
- A Routine Urine Test Has Partial Predictive Value in Premature Rupture of The MembranesDocumento10 páginasA Routine Urine Test Has Partial Predictive Value in Premature Rupture of The Membranesnadya nazwinnAinda não há avaliações
- 10.1007@s12098 020 03412 XDocumento5 páginas10.1007@s12098 020 03412 XOleOhhAinda não há avaliações
- 11 - Trichomonas, Candida, and Gardnerella in CervicalDocumento6 páginas11 - Trichomonas, Candida, and Gardnerella in CervicalRenan RodriguesAinda não há avaliações
- Aborto Septico 2020Documento5 páginasAborto Septico 2020Adrian Pardo VillegasAinda não há avaliações
- DISSEMINATIONDocumento8 páginasDISSEMINATIONAbbireddy SairamAinda não há avaliações
- Preterm Premature Rupture of Membranes: Diagnosis, Evaluation and Management StrategiesDocumento6 páginasPreterm Premature Rupture of Membranes: Diagnosis, Evaluation and Management StrategiesResi Lystianto PutraAinda não há avaliações
- Dont KnowDocumento5 páginasDont KnownawarajAinda não há avaliações
- Multidrug Resistant Uropathogens in Urinary Tract Infections and Their Antibiotic Susceptibility PatternsDocumento4 páginasMultidrug Resistant Uropathogens in Urinary Tract Infections and Their Antibiotic Susceptibility PatternsCERCEL ALESIA IOANAAinda não há avaliações
- Ijpa 18 93Documento7 páginasIjpa 18 93Frank Barreiro SanchezAinda não há avaliações
- Scopus (29) Many2017Documento7 páginasScopus (29) Many2017ika puspitaAinda não há avaliações
- Protective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsDocumento5 páginasProtective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsChika FebrianiAinda não há avaliações
- GGGHHCCCDocumento10 páginasGGGHHCCCNurul Diah AnisaAinda não há avaliações
- Klebsiella Pneumoniae Isolated From Urine ofDocumento9 páginasKlebsiella Pneumoniae Isolated From Urine ofInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Treatment of Asymptomatic Vaginal Candidiasis in Pregnancy To Prevent Preterm Birth An Openlabel Pilot Randomized ContrDocumento7 páginasTreatment of Asymptomatic Vaginal Candidiasis in Pregnancy To Prevent Preterm Birth An Openlabel Pilot Randomized ContrariestianiAinda não há avaliações
- Alger 1988Documento8 páginasAlger 1988Hòa HồAinda não há avaliações
- PresusDocumento6 páginasPresusFrishia DidaAinda não há avaliações
- Neonatal Sepsis in S Asia - A Huge Burden and Spiralling AMRDocumento5 páginasNeonatal Sepsis in S Asia - A Huge Burden and Spiralling AMRdrdrAinda não há avaliações
- Doagnosis Prom 2Documento20 páginasDoagnosis Prom 2Erna Jovem GluberryAinda não há avaliações
- Artigo 03 Filmarray PneumoniaDocumento6 páginasArtigo 03 Filmarray Pneumoniapriscila pimentel martinelliAinda não há avaliações
- The Foot: Original ArticleDocumento5 páginasThe Foot: Original ArticleKarinaayu SerinAinda não há avaliações
- Ureaplasma Urealyticum and Ureaplasma Parvum in Women of Reproductive AgeDocumento17 páginasUreaplasma Urealyticum and Ureaplasma Parvum in Women of Reproductive AgeVivek mandalAinda não há avaliações
- Research Article: Risk Factors and Prevention Strategies of Nosocomial Infection in Geriatric PatientsDocumento6 páginasResearch Article: Risk Factors and Prevention Strategies of Nosocomial Infection in Geriatric Patientschristian demasabuAinda não há avaliações
- Hubungan Tingkat Pengetahuan Kanker Serviks Dengan Minat Untuk Vaksinasi HPV Pada Mahasiswi Fakultas Kedokteran Universitas HKBP Nommensen MedanDocumento4 páginasHubungan Tingkat Pengetahuan Kanker Serviks Dengan Minat Untuk Vaksinasi HPV Pada Mahasiswi Fakultas Kedokteran Universitas HKBP Nommensen Medanintan fairuzAinda não há avaliações
- Trends in Neonatal Septicemia: Emergence of Non-Albicans CandidaDocumento4 páginasTrends in Neonatal Septicemia: Emergence of Non-Albicans CandidaamalanorAinda não há avaliações
- Spectrum of Dysentery in Children Presenting To A Tertiary Level Teaching Hospital in New DelhiDocumento5 páginasSpectrum of Dysentery in Children Presenting To A Tertiary Level Teaching Hospital in New DelhiNasAinda não há avaliações
- Molecular Characterization of Fluconazole Resistant Candida Isolated From Pregnant Women in A Tertiary Healthcare InstitutionDocumento7 páginasMolecular Characterization of Fluconazole Resistant Candida Isolated From Pregnant Women in A Tertiary Healthcare Institutionijmb333Ainda não há avaliações
- Pi Is 0020729213005055Documento4 páginasPi Is 0020729213005055Winna Eka PAinda não há avaliações
- Antimicrobial Sensitivity Pattern in The Mixed Intensive Care Unit in A Tertiary Care Hospital of Eastern NepalDocumento7 páginasAntimicrobial Sensitivity Pattern in The Mixed Intensive Care Unit in A Tertiary Care Hospital of Eastern NepalNilisha PradhanAinda não há avaliações
- Journal 8Documento7 páginasJournal 8margareth silaenAinda não há avaliações
- Knowledge and Practices of Health Workers in Relation To Preeclampsia at Ishaka Adventist Hospital in Western Uganda.Documento9 páginasKnowledge and Practices of Health Workers in Relation To Preeclampsia at Ishaka Adventist Hospital in Western Uganda.KIU PUBLICATION AND EXTENSIONAinda não há avaliações
- Hyun Et Al. 2017 - Efficacy and Safety of TDF To Prevent MTCT of HBVDocumento13 páginasHyun Et Al. 2017 - Efficacy and Safety of TDF To Prevent MTCT of HBVizvery.badAinda não há avaliações
- Children KantiDocumento5 páginasChildren KantiPiyush AcharyaAinda não há avaliações
- 33 - 4 - 07-Dr - KhademDocumento5 páginas33 - 4 - 07-Dr - Khademedy744Ainda não há avaliações
- Candidiasis in PICUDocumento6 páginasCandidiasis in PICUMeirinda HidayantiAinda não há avaliações
- Neisseria Gonorrhea in 1879 (9,10,11,12) - ThisDocumento14 páginasNeisseria Gonorrhea in 1879 (9,10,11,12) - ThisKIU PUBLICATION AND EXTENSIONAinda não há avaliações
- Atencio Azucena Besares Special ProblemDocumento18 páginasAtencio Azucena Besares Special ProblemShane Catherine BesaresAinda não há avaliações
- Chlamydia Antibody Testing Helps in Identifying Females With Possible Tubal Factor InfertilityDocumento6 páginasChlamydia Antibody Testing Helps in Identifying Females With Possible Tubal Factor InfertilityRiany Jade SabrinaAinda não há avaliações
- Life After Amsterdam Placental PathologyDocumento22 páginasLife After Amsterdam Placental PathologyDiego Fernando Ortiz TenorioAinda não há avaliações
- Pandemic and Impact of Covid/ Infectious DiseasesDocumento5 páginasPandemic and Impact of Covid/ Infectious DiseasessamiaAinda não há avaliações
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalAinda não há avaliações
- Endophyte Biotechnology: Potential for Agriculture and PharmacologyNo EverandEndophyte Biotechnology: Potential for Agriculture and PharmacologyAlexander SchoutenAinda não há avaliações
- Journal Acute Necrotizing Ulcerating Gingivitis On HIV PatientDocumento5 páginasJournal Acute Necrotizing Ulcerating Gingivitis On HIV PatientginAinda não há avaliações
- Stevens-Johnson Syndrome Induced by Carbamazepine: PharmacologyDocumento4 páginasStevens-Johnson Syndrome Induced by Carbamazepine: PharmacologyginAinda não há avaliações
- Cellulitis Causes, Symptoms, Treatment - When Should Someone Seek Medical Care For Cellulitis - EMedicineHealthDocumento6 páginasCellulitis Causes, Symptoms, Treatment - When Should Someone Seek Medical Care For Cellulitis - EMedicineHealthginAinda não há avaliações
- Cellulitis - Practice Essentials, Background, PathophysiologyDocumento14 páginasCellulitis - Practice Essentials, Background, PathophysiologyginAinda não há avaliações
- Case ReportDocumento5 páginasCase ReportginAinda não há avaliações
- Irrational Use of DrugDocumento9 páginasIrrational Use of Drugsreedam100% (2)
- Appendices - Archived - Standards and Methods Manual - Food Safety For Industry - Canadian Food Inspection AgencyDocumento21 páginasAppendices - Archived - Standards and Methods Manual - Food Safety For Industry - Canadian Food Inspection Agencymybettafish2020Ainda não há avaliações
- 21 Cephalosp 2015 Mandell Douglas and Bennett S Principles and PracticeDocumento20 páginas21 Cephalosp 2015 Mandell Douglas and Bennett S Principles and PracticeHelen DyAinda não há avaliações
- Dr. Hatem Elgohary Lecturer of General Surgery MD, MrcsDocumento24 páginasDr. Hatem Elgohary Lecturer of General Surgery MD, MrcswinceAinda não há avaliações
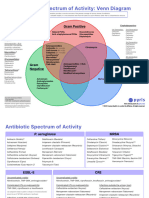
- Antibotics Venn DiagramDocumento2 páginasAntibotics Venn DiagramTop VidsAinda não há avaliações
- Brunei Registered Medicinal ProductsDocumento123 páginasBrunei Registered Medicinal ProductsportosinAinda não há avaliações
- Chapter 5 FT EditedDocumento35 páginasChapter 5 FT EditedPuvenez Tamalantan100% (5)
- NASYTA DIFA FIRDAUS - Tabel Pengelompokkan AntibiotikDocumento1 páginaNASYTA DIFA FIRDAUS - Tabel Pengelompokkan AntibiotikNasyta Difa FirdausAinda não há avaliações
- Tugas Hapalan FarmakologiDocumento5 páginasTugas Hapalan FarmakologiMelda nrmAinda não há avaliações
- Coccidiosis in Poultry: Review On Diagnosis, Control, Prevention and Interaction With Overall Gut HealthDocumento9 páginasCoccidiosis in Poultry: Review On Diagnosis, Control, Prevention and Interaction With Overall Gut HealthRucha ZombadeAinda não há avaliações
- Factors Contributing To Irrational Use of AntibioticsDocumento2 páginasFactors Contributing To Irrational Use of AntibioticsgoyeniranAinda não há avaliações
- Antimicrobial Susceptibility TestingDocumento3 páginasAntimicrobial Susceptibility TestingNoriz Ember DominguezAinda não há avaliações
- Committee On Herbal Medicinal Products (HMPC) : Evaluation of Medicines For Human UseDocumento11 páginasCommittee On Herbal Medicinal Products (HMPC) : Evaluation of Medicines For Human Useroger024Ainda não há avaliações
- BencinDocumento4 páginasBencinimtiazbscAinda não há avaliações
- NCP SinusitisDocumento7 páginasNCP SinusitisBeverly May Ambut71% (7)
- Complete Abstract Book ASTMH - Atlanta 2012-USADocumento3 páginasComplete Abstract Book ASTMH - Atlanta 2012-USAPercy Lezama VigoAinda não há avaliações
- CLSI AST News Update Spring 2016Documento5 páginasCLSI AST News Update Spring 2016ImaneAinda não há avaliações
- Hints For Remembering Medication ClassificationsDocumento2 páginasHints For Remembering Medication ClassificationsSarah SAinda não há avaliações
- We Are Intechopen, Open Access Books: The World'S Leading Publisher of Built by Scientists, For ScientistsDocumento19 páginasWe Are Intechopen, Open Access Books: The World'S Leading Publisher of Built by Scientists, For ScientistsbapaknyanadlirAinda não há avaliações
- Senior Research Scientist Biochemist in NYC NJ Resume Renee ChabinDocumento3 páginasSenior Research Scientist Biochemist in NYC NJ Resume Renee ChabinReneeChabinAinda não há avaliações
- Enrofloxacin: Therapeutic ReviewDocumento4 páginasEnrofloxacin: Therapeutic ReviewAndi Dytha Pramitha SamAinda não há avaliações
- Etanol BacteriaDocumento38 páginasEtanol BacteriaWida YantiAinda não há avaliações
- Jurnal Cefpirome Sulfat PDFDocumento8 páginasJurnal Cefpirome Sulfat PDFd_mayavieAinda não há avaliações
- OXACILLINDocumento1 páginaOXACILLINJust nowAinda não há avaliações
- Treating Osteomyelitis: Antibiotics and Surgery: BackgroundDocumento11 páginasTreating Osteomyelitis: Antibiotics and Surgery: BackgroundCarolina MachadoAinda não há avaliações
- Prisma Health Adult Antimicrobial Guidebook 2021Documento52 páginasPrisma Health Adult Antimicrobial Guidebook 2021JhAinda não há avaliações
- Chapter 9: Infections: Section A: AntibioticsDocumento43 páginasChapter 9: Infections: Section A: AntibioticsAndina NsAinda não há avaliações
- Streptomycin PDFDocumento7 páginasStreptomycin PDFHdjdAinda não há avaliações
- Data Pasien TB JuliDocumento42 páginasData Pasien TB JuliTsubbatun NajahAinda não há avaliações
- Doxicyclin and AcnesDocumento23 páginasDoxicyclin and AcnesRafiqy Sa'adiy FaizunAinda não há avaliações