Você também pode gostar
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionAinda não há avaliações
- HPVDocumento7 páginasHPVWillbourAinda não há avaliações
- Optimizing Cancer Prevention in AdolescentsDocumento4 páginasOptimizing Cancer Prevention in AdolescentsDaniela GuzmánAinda não há avaliações
- Nurses and Midwives Knowledge Attitudes and AcceDocumento11 páginasNurses and Midwives Knowledge Attitudes and AcceGeorge Junior AdomakoAinda não há avaliações
- Nihms 367636Documento12 páginasNihms 367636wonosobo pendampingAinda não há avaliações
- Vecination PregnsDocumento15 páginasVecination PregnsJesus Fernandez AlvarezAinda não há avaliações
- Vacunación Contra El Virus Del Papiloma HumanoDocumento4 páginasVacunación Contra El Virus Del Papiloma HumanoJosé María LauricellaAinda não há avaliações
- Alder Et Al., 2015Documento8 páginasAlder Et Al., 2015Balqis BaslemanAinda não há avaliações
- JSRP 13710Documento45 páginasJSRP 13710Laida Neti MulyaniAinda não há avaliações
- Vaccinations For Pregnant Women: Clinical Expert SeriesDocumento16 páginasVaccinations For Pregnant Women: Clinical Expert SeriesIzzatul YazidahAinda não há avaliações
- VPH CancerDocumento4 páginasVPH CancerJader Aldair Pavon GomezAinda não há avaliações
- Pi Is 0002937807008241Documento7 páginasPi Is 0002937807008241Meita RakhmawatiAinda não há avaliações
- VPH Vaccination - American College of Obstetrician and GynecologyDocumento6 páginasVPH Vaccination - American College of Obstetrician and GynecologyFranz Arturo Lozada HernándezAinda não há avaliações
- Ijgo 12193Documento5 páginasIjgo 12193Aarthi S JayrajAinda não há avaliações
- 1 s2.0 S2590136222000018 MainDocumento12 páginas1 s2.0 S2590136222000018 MainmariaAinda não há avaliações
- Human Papillomavirus Vaccines Who Position Paper May 2017recomme 2017Documento3 páginasHuman Papillomavirus Vaccines Who Position Paper May 2017recomme 2017Putri AlfiraAinda não há avaliações
- Human Papillomavirus Vaccine: Home Study ProgramDocumento18 páginasHuman Papillomavirus Vaccine: Home Study ProgramIswahyudi AlamsyahAinda não há avaliações
- Vacuna HPV Debates - Lippman - Feb08Documento4 páginasVacuna HPV Debates - Lippman - Feb08api-26512586Ainda não há avaliações
- Vaksinasi HPVDocumento6 páginasVaksinasi HPVCarissa ChungAinda não há avaliações
- Annals of Medicine HPVDocumento12 páginasAnnals of Medicine HPVJacqueline MarieAinda não há avaliações
- Cervical Cancer - An Overview of Pathophysiology and ManagementDocumento9 páginasCervical Cancer - An Overview of Pathophysiology and ManagementIndah 15Ainda não há avaliações
- Proposal AnneDocumento14 páginasProposal AnneLakshmi RjAinda não há avaliações
- Vaccination JournalDocumento10 páginasVaccination JournalJemimah Keziah Bandiwan BannaweAinda não há avaliações
- Journal PUBMEDDocumento6 páginasJournal PUBMEDRestu RahmanAinda não há avaliações
- Hiv in Pregnancy Literature ReviewDocumento7 páginasHiv in Pregnancy Literature Reviewafmztwoalwbteq100% (1)
- JurnalDocumento16 páginasJurnalTrysna Ayu SukardiAinda não há avaliações
- Chapter 15: HPV Vaccine Use in The Developing WorldDocumento8 páginasChapter 15: HPV Vaccine Use in The Developing Worldhst939Ainda não há avaliações
- Qi PlanDocumento7 páginasQi Planapi-661765354Ainda não há avaliações
- Final Compilation - Group D ProjectDocumento75 páginasFinal Compilation - Group D ProjectRukaiya Auwal AliAinda não há avaliações
- 02 - 03 - Oral-And-Maxillofacial-Pathology - Cancer Prevention Through HPV Vaccination For Dental Health Care ProvidersDocumento8 páginas02 - 03 - Oral-And-Maxillofacial-Pathology - Cancer Prevention Through HPV Vaccination For Dental Health Care Providersamirmahdi82.s.fAinda não há avaliações
- HIV and Pregnancy: How To Manage Conflicting Recommendations From Evidence-Based GuidelinesDocumento6 páginasHIV and Pregnancy: How To Manage Conflicting Recommendations From Evidence-Based GuidelinesIsmaelJoséGonzálezGuzmánAinda não há avaliações
- HPV-Vaccine Hesitancy in Colombia A Mixed-Methods StudyDocumento16 páginasHPV-Vaccine Hesitancy in Colombia A Mixed-Methods Studyandrea sanabria pedrazaAinda não há avaliações
- Briefing NoteDocumento3 páginasBriefing Noteapi-508465569Ainda não há avaliações
- Literature Review HPV VaccineDocumento7 páginasLiterature Review HPV Vaccinegw32pesz100% (1)
- Improving Adolescent Health: Focus On HPV Vaccine AcceptanceDocumento7 páginasImproving Adolescent Health: Focus On HPV Vaccine AcceptanceYudha SatriaAinda não há avaliações
- Seminars in Oncology NursingDocumento9 páginasSeminars in Oncology NursingangelitostorresitosAinda não há avaliações
- Awareness of HPV and HPV Vaccines, Acceptance To VDocumento6 páginasAwareness of HPV and HPV Vaccines, Acceptance To VMa. Isabel LadiaAinda não há avaliações
- Vaksin VarelaDocumento8 páginasVaksin VarelaPutra EkaAinda não há avaliações
- Chapter 25: Education, Training, and Communication For HPV VaccinesDocumento9 páginasChapter 25: Education, Training, and Communication For HPV Vaccineshst939Ainda não há avaliações
- Keywords: Human Papillomavirus Vaccine, Efficacy, Safety, Phase III Randomized TrialsDocumento10 páginasKeywords: Human Papillomavirus Vaccine, Efficacy, Safety, Phase III Randomized TrialsBassment MixshowAinda não há avaliações
- Will HPV Vaccination Prevent Cervical Cancer?: Claire P Rees, Petra Brhlikova and Allyson M PollockDocumento15 páginasWill HPV Vaccination Prevent Cervical Cancer?: Claire P Rees, Petra Brhlikova and Allyson M PollockGina Ionescu AnculeteAinda não há avaliações
- Article About HPVDocumento32 páginasArticle About HPVriza susramaAinda não há avaliações
- Pediatr Clin North Am 2023 Tabla de ContenidoDocumento4 páginasPediatr Clin North Am 2023 Tabla de ContenidocdsaludAinda não há avaliações
- Effectiveness of Investments in Leadership and Management Capacity in Thecontext of National Epi ProgramsDocumento2 páginasEffectiveness of Investments in Leadership and Management Capacity in Thecontext of National Epi ProgramsZheefAinda não há avaliações
- PIIS2214109X24000093Documento2 páginasPIIS2214109X24000093MesutHasipiAinda não há avaliações
- A Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in The PhilippinesDocumento17 páginasA Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in The PhilippinesYukiko CalimutanAinda não há avaliações
- Thesis On HPV VaccineDocumento8 páginasThesis On HPV Vaccinegjftqhnp100% (2)
- Hoes 2022Documento11 páginasHoes 2022contreraz7Ainda não há avaliações
- Book 1 Cancer CervikDocumento20 páginasBook 1 Cancer CervikihsansabridrAinda não há avaliações
- Vaccination Against Cervical Cancer2998Documento22 páginasVaccination Against Cervical Cancer2998Krishnaveni MurugeshAinda não há avaliações
- Human Papilloma Virus Vaccine For Cervical Cancer PreventionDocumento9 páginasHuman Papilloma Virus Vaccine For Cervical Cancer Preventionsayeef khanAinda não há avaliações
- Committee Opinion: Human Papillomavirus VaccinationDocumento7 páginasCommittee Opinion: Human Papillomavirus VaccinationHugo ChavezAinda não há avaliações
- Peer Review HatchDocumento3 páginasPeer Review Hatchapi-680921549Ainda não há avaliações
- Research Paper On Childhood VaccinationsDocumento8 páginasResearch Paper On Childhood Vaccinationsefjr9yx3100% (1)
- Obstetric Care in Patients With HIV DiseaseDocumento10 páginasObstetric Care in Patients With HIV DiseaseJulie Carnetion DAinda não há avaliações
- Vaccine HesitancyDocumento12 páginasVaccine HesitancyMhd HidayattullahAinda não há avaliações
- Interventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsDocumento10 páginasInterventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsMariaAinda não há avaliações
- The Prevention Program of Cervical CanceDocumento6 páginasThe Prevention Program of Cervical Cancepb.nakulaAinda não há avaliações
- 9 Catcup Imun ReviewDocumento18 páginas9 Catcup Imun ReviewErna MiraniAinda não há avaliações
- VasavanSharangi Assign2Documento11 páginasVasavanSharangi Assign2sharangiivAinda não há avaliações
- The Minitube Group: Dr. Monika EschDocumento45 páginasThe Minitube Group: Dr. Monika EschRyan SadonoAinda não há avaliações
- J Clin Pathol 1988 Crocker 576 81Documento7 páginasJ Clin Pathol 1988 Crocker 576 81Ryan SadonoAinda não há avaliações
- The Minitube Group: Dr. Monika EschDocumento45 páginasThe Minitube Group: Dr. Monika EschRyan SadonoAinda não há avaliações
- FullPIERS Paper-LancetDocumento39 páginasFullPIERS Paper-LancetRyan SadonoAinda não há avaliações
- What Is New in Diabetes in PregnancyDocumento2 páginasWhat Is New in Diabetes in PregnancyRyan SadonoAinda não há avaliações
- Optimizing Natural FertilityDocumento7 páginasOptimizing Natural FertilityRyan SadonoAinda não há avaliações
- 15 02 UpdateFetalTherapy 0Documento59 páginas15 02 UpdateFetalTherapy 0Ryan SadonoAinda não há avaliações
- What Is AdenomyosisDocumento2 páginasWhat Is AdenomyosisRyan SadonoAinda não há avaliações
- Ethical Considerations of Fetal TherapyDocumento13 páginasEthical Considerations of Fetal TherapyRyan SadonoAinda não há avaliações
- Premature Labour Clinical GuidelineDocumento7 páginasPremature Labour Clinical GuidelineRyan SadonoAinda não há avaliações
- Bladder PDFDocumento22 páginasBladder PDFSuci Mega SariAinda não há avaliações
- Carlie's Story: by Tami Perez-MesaDocumento6 páginasCarlie's Story: by Tami Perez-MesaJennifer HeinAinda não há avaliações
- Self Study Intraoral Anatomy RadiologyDocumento80 páginasSelf Study Intraoral Anatomy RadiologydeenmAinda não há avaliações
- Indexed Journals of Pakistan - Medline and EmbaseDocumento48 páginasIndexed Journals of Pakistan - Medline and EmbaseFaisal RoohiAinda não há avaliações
- Developmental Assessment of Hospitalized ChildDocumento11 páginasDevelopmental Assessment of Hospitalized ChildmcowellAinda não há avaliações
- Symptom Based RadiologyDocumento3 páginasSymptom Based Radiologydgina8800Ainda não há avaliações
- Dopamine Vs EpinephrineDocumento11 páginasDopamine Vs EpinephrineAyiek WicaksonoAinda não há avaliações
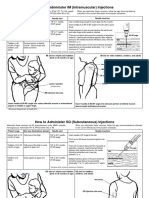
- Im SQ Admin PDFDocumento2 páginasIm SQ Admin PDFAlvin JjAinda não há avaliações
- Child Asthma Action PlanDocumento2 páginasChild Asthma Action PlanMinerva StanciuAinda não há avaliações
- Interproximal Height of BoneDocumento3 páginasInterproximal Height of Bonefinislux1Ainda não há avaliações
- Find Best Specialist Doctor List in Dhaka BangladeshDocumento4 páginasFind Best Specialist Doctor List in Dhaka BangladeshHealth ProfileAinda não há avaliações
- Patch Adams 02Documento3 páginasPatch Adams 02api-3750171Ainda não há avaliações
- Developmental DefectsDocumento16 páginasDevelopmental DefectsdeenmAinda não há avaliações
- Pediatrics 1981 Versmold 607 13Documento9 páginasPediatrics 1981 Versmold 607 13Andrés AcevedoAinda não há avaliações
- Acute Nephrology For The Critical Care Physician 2015th EditionDocumento280 páginasAcute Nephrology For The Critical Care Physician 2015th EditionHiago Sousa100% (1)
- Neonatal Cns ExaminationDocumento33 páginasNeonatal Cns ExaminationShishir KumarAinda não há avaliações
- International Journal of Biological & Medical Research: Case ReportDocumento3 páginasInternational Journal of Biological & Medical Research: Case ReportAndreea Diana DrăgoiAinda não há avaliações
- Ada 2020 PDFDocumento224 páginasAda 2020 PDFWinston SanjayaAinda não há avaliações
- AVPUDocumento2 páginasAVPUAnissa Citra DewiAinda não há avaliações
- TeresaDocumento2 páginasTeresaapi-435131948Ainda não há avaliações
- ACCREDITED PEDIA ON Chong Hua Hospital Mandaue & Cancer CenterDocumento6 páginasACCREDITED PEDIA ON Chong Hua Hospital Mandaue & Cancer CenterBrenna BiancaAinda não há avaliações
- Bacterial Sepsis in PregnancyDocumento14 páginasBacterial Sepsis in PregnancydraasfourAinda não há avaliações
- My Article B AngleDocumento4 páginasMy Article B AngleNiyati VerulkarAinda não há avaliações
- Jurnal AppDocumento19 páginasJurnal AppDira RiskaAinda não há avaliações
- EncephalitisDocumento27 páginasEncephalitisHasRoni Fathurrahman100% (1)
- Labour Analgesia - Recent ConceptsDocumento18 páginasLabour Analgesia - Recent ConceptsSuresh KumarAinda não há avaliações
- Patient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)Documento15 páginasPatient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)krh5fnjnprAinda não há avaliações
- Git & Nutrition McqsDocumento24 páginasGit & Nutrition McqsShahabuddin Shaikh100% (1)
- VMU BrochureDocumento15 páginasVMU BrochurekarthiktaraAinda não há avaliações
- CMS Neuro Form Number 4 Query Answer Req? - USMLE Forum: Jun 30, 2016 - 7 PostsDocumento3 páginasCMS Neuro Form Number 4 Query Answer Req? - USMLE Forum: Jun 30, 2016 - 7 Postsbob0% (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 4.5 de 5 estrelas4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4.5 de 5 estrelas4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNo EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNota: 3.5 de 5 estrelas3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceNo EverandTo Explain the World: The Discovery of Modern ScienceNota: 3.5 de 5 estrelas3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsNo EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsNota: 4.5 de 5 estrelas4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingNo EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingNota: 4 de 5 estrelas4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)