Você também pode gostar
- Daftar Obat Puskes MerdekaDocumento2 páginasDaftar Obat Puskes MerdekaAnonymous aH8gCZ7zjAinda não há avaliações
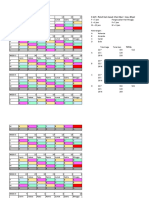
- 3 Shift: Pola 3 Hari Masuk 1 Hari Libur + Max. 40 Jam/mingguDocumento4 páginas3 Shift: Pola 3 Hari Masuk 1 Hari Libur + Max. 40 Jam/mingguAnonymous aH8gCZ7zjAinda não há avaliações
- Research Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisDocumento10 páginasResearch Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisAnonymous aH8gCZ7zjAinda não há avaliações
- ID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFDocumento10 páginasID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFAnonymous aH8gCZ7zjAinda não há avaliações
- Case HemoroidDocumento19 páginasCase HemoroidAnonymous aH8gCZ7zjAinda não há avaliações
- IT 3 - Spinal Cord InjuryDocumento38 páginasIT 3 - Spinal Cord InjuryAnonymous aH8gCZ7zjAinda não há avaliações
- Excercise 2 - Frequency MeasureDocumento6 páginasExcercise 2 - Frequency MeasureAnonymous aH8gCZ7zj75% (4)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Lecture2 v1Documento69 páginasLecture2 v1c.ronaldo2012777Ainda não há avaliações
- Chem 3052 CHAPTER 7 (Nuclear Magnetic Resonance Spectroscopy (NMR) )Documento6 páginasChem 3052 CHAPTER 7 (Nuclear Magnetic Resonance Spectroscopy (NMR) )ashenafiAinda não há avaliações
- Pump Shotgun: Instruction ManualDocumento5 páginasPump Shotgun: Instruction ManualJustinAinda não há avaliações
- Ligamentele LargiDocumento2 páginasLigamentele LargiIoana IonicaAinda não há avaliações
- PricelistDocumento4 páginasPricelistMAYMART CASABAAinda não há avaliações
- Curvature CorrectionDocumento7 páginasCurvature CorrectionE J SAinda não há avaliações
- Traffic Cases in GSMDocumento18 páginasTraffic Cases in GSMkamal100% (1)
- Product CatalogDocumento4 páginasProduct CatalogpeejayjacintoAinda não há avaliações
- 2020 Landfill Capacity Calculation Work SheetDocumento4 páginas2020 Landfill Capacity Calculation Work SheetLYAinda não há avaliações
- 06ESL37 Analog Electronics Lab MANUALDocumento70 páginas06ESL37 Analog Electronics Lab MANUALSan AngadiAinda não há avaliações
- Proposal Form NagDocumento1 páginaProposal Form Nagnitheesh kumarAinda não há avaliações
- Acc05 SCG116Documento42 páginasAcc05 SCG116Hilal HazaaAinda não há avaliações
- Barium Chloride 2h2o LRG MsdsDocumento3 páginasBarium Chloride 2h2o LRG MsdsAnas GiselAinda não há avaliações
- Production System: BY: Mallick MD Fahad Roll No. 16Documento36 páginasProduction System: BY: Mallick MD Fahad Roll No. 16Fahad SailorAinda não há avaliações
- Backlash SDPDocumento11 páginasBacklash SDPPatrick Cyr GagnéAinda não há avaliações
- Free-Field Equivalent Localization of Virtual AudioDocumento9 páginasFree-Field Equivalent Localization of Virtual AudiojulianpalacinoAinda não há avaliações
- Fuk SecDocumento1 páginaFuk SecHirushan MenukaAinda não há avaliações
- The Use of Proton Pump Inhibitors in Treating and Preventing NSAID-induced Mucosal DamageDocumento6 páginasThe Use of Proton Pump Inhibitors in Treating and Preventing NSAID-induced Mucosal DamageFriska Rachmanita PrayogoAinda não há avaliações
- Samuelson and Nordhaus ch22 PDFDocumento30 páginasSamuelson and Nordhaus ch22 PDFVictor ManatadAinda não há avaliações
- PPP-B-676 e PDFDocumento34 páginasPPP-B-676 e PDFffincher4203Ainda não há avaliações
- Fluid Mechanics & Machines - by LearnEngineering - inDocumento307 páginasFluid Mechanics & Machines - by LearnEngineering - inVishva PatelAinda não há avaliações
- Infineon IRFZ44N DataSheet v01 - 01 ENDocumento9 páginasInfineon IRFZ44N DataSheet v01 - 01 ENIkram RidhoAinda não há avaliações
- The Church of Kapnikarea in Athens - N. GkiolesDocumento13 páginasThe Church of Kapnikarea in Athens - N. GkiolesMaronasAinda não há avaliações
- NSTM.512v0.FANS.S9086 RS STM 010 CH 512R21Sep99Documento60 páginasNSTM.512v0.FANS.S9086 RS STM 010 CH 512R21Sep99jwfqcw74mfAinda não há avaliações
- Grocery GatewayDocumento2 páginasGrocery GatewayKumari Mohan0% (2)
- Module III Rural MarketingDocumento30 páginasModule III Rural MarketingNikita YadavAinda não há avaliações
- An Infallible JusticeDocumento7 páginasAn Infallible JusticeMani Gopal DasAinda não há avaliações
- Stock+List 6ct8.3g2 Esn#30549237 Cpl#2218 GeneradorDocumento34 páginasStock+List 6ct8.3g2 Esn#30549237 Cpl#2218 GeneradorAlexis SanchezAinda não há avaliações
- 1753-Article Text-39640-3-10-20220815Documento9 páginas1753-Article Text-39640-3-10-20220815Inah SaritaAinda não há avaliações
- Citadel of Kirkuk 1Documento17 páginasCitadel of Kirkuk 1ArézAzadAinda não há avaliações