Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Yijin Jing Chinese Health AssocDocumento12 páginasYijin Jing Chinese Health Assoctansoei100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Etextbook PDF For Principles of Anatomy and Physiology 15th EditionDocumento61 páginasEtextbook PDF For Principles of Anatomy and Physiology 15th Editionkarla.woodruff227100% (45)
- 1st Quarter Exam - ScienceDocumento4 páginas1st Quarter Exam - ScienceMeljean Kalaw Castillo100% (1)
- Physical Therapy Documentation Templates PDFDocumento6 páginasPhysical Therapy Documentation Templates PDFNellAinda não há avaliações
- Ccypi 3.0Documento76 páginasCcypi 3.0GirishAinda não há avaliações
- COPD PathophysiologyDocumento1 páginaCOPD PathophysiologyJustin Ahorro-Dionisio33% (3)
- NCP & Prio!!!Documento45 páginasNCP & Prio!!!Sj 斗力上100% (1)
- Ajay YadavDocumento351 páginasAjay YadavTabish Javaid90% (10)
- Biology 8 Frog Dissection GuideDocumento10 páginasBiology 8 Frog Dissection GuideRyan SantosAinda não há avaliações
- Spirometry ReportDocumento11 páginasSpirometry ReportTharshini_Indr_6713100% (1)
- Adan-Flow Cytometry-Basic Principles and ApplicationsDocumento15 páginasAdan-Flow Cytometry-Basic Principles and ApplicationsArnab Ghosh100% (1)
- The Women's Fitness Book PDFDocumento338 páginasThe Women's Fitness Book PDFargent80% (5)
- Technical Manual GN Advance Neo and TSDocumento168 páginasTechnical Manual GN Advance Neo and TSReuel Tacay100% (1)
- Chronic Generalized Dermatophilosis in A BuffaloDocumento3 páginasChronic Generalized Dermatophilosis in A BuffaloHendroAinda não há avaliações
- Assessment of Endometritis in Arabian MareDocumento5 páginasAssessment of Endometritis in Arabian MareHendroAinda não há avaliações
- My ThesisDocumento144 páginasMy ThesisHendroAinda não há avaliações
- El Cig PDFDocumento9 páginasEl Cig PDFHendroAinda não há avaliações
- Analy Nicot' PDFDocumento16 páginasAnaly Nicot' PDFHendroAinda não há avaliações
- El Cig PDFDocumento9 páginasEl Cig PDFHendroAinda não há avaliações
- Komponen Vapor PDFDocumento28 páginasKomponen Vapor PDFHendroAinda não há avaliações
- Sheep & Goat Pox: ImportanceDocumento4 páginasSheep & Goat Pox: ImportanceHendroAinda não há avaliações
- Bismuth SubsalicylateDocumento7 páginasBismuth SubsalicylateHendroAinda não há avaliações
- Measurement of Tumor Necrosis Factor Activity Flow CytometryDocumento4 páginasMeasurement of Tumor Necrosis Factor Activity Flow CytometryHendroAinda não há avaliações
- TTNFF PDFDocumento7 páginasTTNFF PDFHendroAinda não há avaliações
- TTNFF PDFDocumento7 páginasTTNFF PDFHendroAinda não há avaliações
- TNF and FowDocumento12 páginasTNF and FowHendroAinda não há avaliações
- TNF and FowDocumento12 páginasTNF and FowHendroAinda não há avaliações
- 216 616 1 PBDocumento12 páginas216 616 1 PBHendroAinda não há avaliações
- Hypocalcemia in Aged: Herd of BeefDocumento2 páginasHypocalcemia in Aged: Herd of BeefHendroAinda não há avaliações
- 216 616 1 PBDocumento8 páginas216 616 1 PBYasserAlChemistAinda não há avaliações
- I L Obat-Alat-Peternakan PDFDocumento3 páginasI L Obat-Alat-Peternakan PDFHendroAinda não há avaliações
- Hypocalcemia in Aged: Herd of BeefDocumento2 páginasHypocalcemia in Aged: Herd of BeefHendroAinda não há avaliações
- Disordersof Calciumhypercalcemiahypocalcemia Dibartola Fluid Electrolytes 3 RD 2006Documento74 páginasDisordersof Calciumhypercalcemiahypocalcemia Dibartola Fluid Electrolytes 3 RD 2006Hendro100% (1)
- 216 616 1 PBDocumento12 páginas216 616 1 PBHendroAinda não há avaliações
- Handling, RestrainDocumento96 páginasHandling, RestrainHendroAinda não há avaliações
- An Experimental Study of The Pathogenicity of A Duck Hepatitis A Virus Genotype C Isolate in Specific Pathogen Free DucklingsDocumento9 páginasAn Experimental Study of The Pathogenicity of A Duck Hepatitis A Virus Genotype C Isolate in Specific Pathogen Free DucklingsHendroAinda não há avaliações
- PankreasDocumento10 páginasPankreasHendroAinda não há avaliações
- Nutritional Disorders in Beef Cattle: Agriculture and Natural ResourcesDocumento8 páginasNutritional Disorders in Beef Cattle: Agriculture and Natural ResourcesHendroAinda não há avaliações
- Strategies For Preventing Milk Fever in Dairy CattleDocumento13 páginasStrategies For Preventing Milk Fever in Dairy CattleHendroAinda não há avaliações
- Duck Virus Hepatitis: OIE Terrestrial Manual 2008 515Documento9 páginasDuck Virus Hepatitis: OIE Terrestrial Manual 2008 515HendroAinda não há avaliações
- Handling, RestrainDocumento96 páginasHandling, RestrainHendroAinda não há avaliações
- Unit 5 Anatomy and Physiology in Health and Social CareDocumento53 páginasUnit 5 Anatomy and Physiology in Health and Social Caremurdatwotimes90% (31)
- Congenital Lobar EmphysemaDocumento25 páginasCongenital Lobar Emphysemasheme1711Ainda não há avaliações
- Comparative Respiratory SystemDocumento12 páginasComparative Respiratory Systemlinnet17Ainda não há avaliações
- Material Safety Data Sheet For Nickel Cadium BatteryDocumento3 páginasMaterial Safety Data Sheet For Nickel Cadium BatteryM Usman ChaudharyAinda não há avaliações
- Punthmatharith Et Coll (2018) - DONEDocumento14 páginasPunthmatharith Et Coll (2018) - DONEMaya HammoudAinda não há avaliações
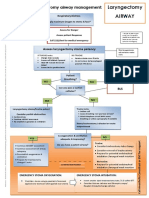
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocumento1 páginaLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieAinda não há avaliações
- Transient Tachypnea of The Newborn: BackgroundDocumento9 páginasTransient Tachypnea of The Newborn: BackgroundAnnisa YusufAinda não há avaliações
- Respiratory System AssignmentDocumento3 páginasRespiratory System AssignmentzainaAinda não há avaliações
- Transient TachypneaDocumento3 páginasTransient TachypneaChristopher Balictar HilisAinda não há avaliações
- S3 Breathing SystemDocumento18 páginasS3 Breathing System廖思明Ainda não há avaliações
- Acute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsDocumento2 páginasAcute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsSachin SinghAinda não há avaliações
- Respiratory System SongDocumento1 páginaRespiratory System SongfsuhariAinda não há avaliações
- Lewis Heart Failure Care PlanDocumento4 páginasLewis Heart Failure Care Plansarahbearcoups100% (1)
- Mechanisms of Hypoxemia: Review ArticleDocumento14 páginasMechanisms of Hypoxemia: Review ArticleJhon CruzAinda não há avaliações
- YogabookDocumento36 páginasYogabookDipesh ParekhAinda não há avaliações
- Internet of Things For Smart Healthcare: Technologies, Challenges, and OpportunitiesDocumento24 páginasInternet of Things For Smart Healthcare: Technologies, Challenges, and OpportunitiesSriharsha SarmaAinda não há avaliações
- Makalah Phonology Kelompok 2Documento11 páginasMakalah Phonology Kelompok 2meldianto manugalaAinda não há avaliações
- Folio Biology A+Documento67 páginasFolio Biology A+Nina IsmailAinda não há avaliações