Você também pode gostar
- Animal Management in Disasters, Volume 1, Animals and PeopleNo EverandAnimal Management in Disasters, Volume 1, Animals and PeopleAinda não há avaliações
- The Perception of Disaster Preparedness Among Filipino Nursing StudentsDocumento135 páginasThe Perception of Disaster Preparedness Among Filipino Nursing StudentsReginald Don Destura100% (3)
- Disaster Preparedness in Philippine Nurses: World HealthDocumento9 páginasDisaster Preparedness in Philippine Nurses: World HealthTiwi Dewi WulanAinda não há avaliações
- Attitude ScaleDocumento15 páginasAttitude ScaleJones PhoneAinda não há avaliações
- Nurses' Perception of Disaster: Implications For Disaster Nursing CurriculumDocumento8 páginasNurses' Perception of Disaster: Implications For Disaster Nursing CurriculumJbl2328Ainda não há avaliações
- OutlineDocumento2 páginasOutlineLea CaringalAinda não há avaliações
- Evaluation of Disaster Preparedness and Perceived Barriers Among Student Nurses. IDocumento3 páginasEvaluation of Disaster Preparedness and Perceived Barriers Among Student Nurses. IAngelica Joy AbadAinda não há avaliações
- Educating Nursing Students On Emergency Preparedness - A Pilot ProDocumento57 páginasEducating Nursing Students On Emergency Preparedness - A Pilot ProTiwi Dewi WulanAinda não há avaliações
- Review of Related Literature and StudiesDocumento7 páginasReview of Related Literature and StudiesJersie Mae G. FabieAinda não há avaliações
- Unit 1& 2 Disaster MGTDocumento32 páginasUnit 1& 2 Disaster MGTAarti SainiAinda não há avaliações
- Thesis Paraphrased Chap 2Documento17 páginasThesis Paraphrased Chap 2Bibi100% (1)
- Nurses RoleDocumento14 páginasNurses RolesweetpeaAinda não há avaliações
- Common Myths and Fallacies in Disaster Medicine: An Evidence-Based ReviewDocumento12 páginasCommon Myths and Fallacies in Disaster Medicine: An Evidence-Based ReviewNuratri HarmianiAinda não há avaliações
- Knowledge and Skills of Emergency Care During Disaster For Community Health Volunteers: A Literature ReviewDocumento11 páginasKnowledge and Skills of Emergency Care During Disaster For Community Health Volunteers: A Literature ReviewZACHARIAH MANKIRAinda não há avaliações
- Research Chapter 1Documento20 páginasResearch Chapter 1MidaRadamAinda não há avaliações
- Global IssueDocumento2 páginasGlobal IssueCkaye GansubinAinda não há avaliações
- Nurses Knowledge and Practices Regarding Disasters Management and Emergency PreparednessDocumento13 páginasNurses Knowledge and Practices Regarding Disasters Management and Emergency PreparednessZACHARIAH MANKIRAinda não há avaliações
- Fung Et - Al.Documento6 páginasFung Et - Al.Noi Mae NebreaAinda não há avaliações
- C Millet Post Ver 073113Documento37 páginasC Millet Post Ver 073113Ferry Nirwana Ade SaputraAinda não há avaliações
- Disaster Nursing - SeminarDocumento41 páginasDisaster Nursing - SeminarVjesh V Mohan100% (12)
- 4 1 1 An Analysis On Rapid AssessmentDocumento4 páginas4 1 1 An Analysis On Rapid AssessmentHannah DuyagAinda não há avaliações
- The Role, Preparedness and Management of Nurses During Disasters 1325648617Documento26 páginasThe Role, Preparedness and Management of Nurses During Disasters 1325648617Pepper Mint0% (1)
- Disaster Assignment 100Documento4 páginasDisaster Assignment 100Hassan Muhammad YounasAinda não há avaliações
- Nurses' Preparedness and Perceived Competence in Managing DisastersDocumento8 páginasNurses' Preparedness and Perceived Competence in Managing DisastersJbl2328Ainda não há avaliações
- Munasinghe2019 HHHDocumento10 páginasMunasinghe2019 HHHAnna HAinda não há avaliações
- Disaster Preparedness in Philippine Nurses: World HealthDocumento8 páginasDisaster Preparedness in Philippine Nurses: World HealthBudi WidiyantoAinda não há avaliações
- Manajemen Bencana PDFDocumento16 páginasManajemen Bencana PDFMuhammad Ichsan MustariAinda não há avaliações
- Healthcare Facility Preparedness in DisasterDocumento16 páginasHealthcare Facility Preparedness in DisasterydtrgnAinda não há avaliações
- Revised Research ZoomDocumento51 páginasRevised Research ZoomAubrey Unique EvangelistaAinda não há avaliações
- A Study To Assess Awareness On Disaster Management Among School Going Children in Gwalior (M.P.)Documento5 páginasA Study To Assess Awareness On Disaster Management Among School Going Children in Gwalior (M.P.)Mohaimen macodAinda não há avaliações
- Importance of D MDocumento3 páginasImportance of D MpankajkapseAinda não há avaliações
- Teaching Disaster Nursing by Utilizing The Jennings Disaster Nursing Management ModelDocumento9 páginasTeaching Disaster Nursing by Utilizing The Jennings Disaster Nursing Management Modelyuihan oshiAinda não há avaliações
- Combating Urban Hazard A Qualitative Study On The Perception On Disaster Preparedness of STEM StudentsDocumento43 páginasCombating Urban Hazard A Qualitative Study On The Perception On Disaster Preparedness of STEM StudentsChlarisse Gabrielle TanAinda não há avaliações
- Disaster Risk Management-Awareness and Preparedness A Term PaperDocumento32 páginasDisaster Risk Management-Awareness and Preparedness A Term PaperjaymarmandiaAinda não há avaliações
- Disaster PreparednessDocumento13 páginasDisaster PreparednessLeodoro LabragueAinda não há avaliações
- Disaster Management in Pakistan EssayDocumento13 páginasDisaster Management in Pakistan EssayGrand chemistryAinda não há avaliações
- Disaster 2Documento16 páginasDisaster 2ALJHON OSORIOAinda não há avaliações
- Out 9Documento17 páginasOut 9hikmat pramajatiAinda não há avaliações
- Disaster: Natural DisastersDocumento6 páginasDisaster: Natural Disastersmary joy banaresAinda não há avaliações
- Disaster Management:: The Role and Preparedness of Veterinary ServicesDocumento14 páginasDisaster Management:: The Role and Preparedness of Veterinary ServicesShafakatAinda não há avaliações
- Local ArticlesDocumento5 páginasLocal ArticlesJhomaliah DaitAinda não há avaliações
- Chapter I, II, III, IV, V FinalDocumento31 páginasChapter I, II, III, IV, V FinalNhor Jehan SaydinAinda não há avaliações
- PHC and EmergeincyDocumento16 páginasPHC and EmergeincyNasteexa Abdulaahi AbshirAinda não há avaliações
- APEDNN Curricular Framework in Emergency and Disaster Nursing - Sept2009Documento35 páginasAPEDNN Curricular Framework in Emergency and Disaster Nursing - Sept2009janus5zu5iga5de5leonAinda não há avaliações
- DISASTER PREPAREDNESS OF MUNICIPALITY OF MAAYON Latumbo - EditedDocumento18 páginasDISASTER PREPAREDNESS OF MUNICIPALITY OF MAAYON Latumbo - Editedkinrosario02Ainda não há avaliações
- Zamboangacity State Polytechnic College Graduate SchoolDocumento10 páginasZamboangacity State Polytechnic College Graduate SchoolJoanes OcamiaAinda não há avaliações
- Al., 2011) - It Is Thus Expedient To Prepare The Public Health Nursing Work-Force WithinDocumento9 páginasAl., 2011) - It Is Thus Expedient To Prepare The Public Health Nursing Work-Force Withindyan ayu puspariniAinda não há avaliações
- 731-Article Text-2299-2-10-20220905Documento31 páginas731-Article Text-2299-2-10-20220905Pachut ChayAinda não há avaliações
- Justification of The StudyDocumento1 páginaJustification of The StudyMaria MiguelAinda não há avaliações
- Ratna Wahyu FDocumento14 páginasRatna Wahyu FTria Rosa RomadhonaAinda não há avaliações
- DisasterDocumento61 páginasDisasterHyndavi Marella100% (1)
- 27 A. Undergrad - Disaster ManagementDocumento44 páginas27 A. Undergrad - Disaster ManagementLorenz SmallAinda não há avaliações
- Thesis Title About Disaster PreparednessDocumento4 páginasThesis Title About Disaster Preparednessfbyx8sck100% (2)
- Disasters-Natural: Go ToDocumento10 páginasDisasters-Natural: Go Toiricamae ciervoAinda não há avaliações
- Nursing DisasterDocumento10 páginasNursing DisasterReymon Jan RodadoAinda não há avaliações
- ICN Framework of Disaster Nursing CompetenciesDocumento27 páginasICN Framework of Disaster Nursing CompetenciesChannelG100% (1)
- 01 Jurnal BellaDocumento13 páginas01 Jurnal BellaBella Bri KitaAinda não há avaliações
- JurnalDocumento10 páginasJurnaldyahAinda não há avaliações
- Emergency Preparedness in Obstetrics: Clinical Expert SeriesDocumento12 páginasEmergency Preparedness in Obstetrics: Clinical Expert Seriesgilbert setiawanAinda não há avaliações
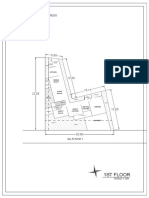
- 1St Floor: House On Paus Schematic Plan ProgressDocumento2 páginas1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaAinda não há avaliações
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocumento11 páginasSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaAinda não há avaliações
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyDocumento10 páginasDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaAinda não há avaliações
- Gibson 2010Documento19 páginasGibson 2010fiora.ladesvitaAinda não há avaliações
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocumento12 páginasChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaAinda não há avaliações
- Ambulatory Care Nursing: Coming Soon!Documento16 páginasAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaAinda não há avaliações
- Medicalscience: EcancerDocumento7 páginasMedicalscience: Ecancerfiora.ladesvitaAinda não há avaliações
- Caring: Prof. Dr. Budi Anna Keliat, MappscDocumento59 páginasCaring: Prof. Dr. Budi Anna Keliat, Mappscfiora.ladesvitaAinda não há avaliações
- Assessment Rating ScaleDocumento8 páginasAssessment Rating Scalefiora.ladesvitaAinda não há avaliações
- Anderson2004 PDFDocumento7 páginasAnderson2004 PDFfiora.ladesvitaAinda não há avaliações
- Sistematic Review HoneyDocumento159 páginasSistematic Review Honeyfiora.ladesvitaAinda não há avaliações
- Living With Kidney DiseaseDocumento96 páginasLiving With Kidney Diseasefiora.ladesvitaAinda não há avaliações
- Idiom Meaning Examples: Toefl PreparationDocumento4 páginasIdiom Meaning Examples: Toefl Preparationfiora.ladesvitaAinda não há avaliações
- Care PlanDocumento4 páginasCare Planapi-217086261Ainda não há avaliações
- What Is Personal HygieneDocumento4 páginasWhat Is Personal HygieneAnonymous 0FWhoTu100% (1)
- Gay Issue A Century AgoDocumento4 páginasGay Issue A Century AgoElla Jane EngoAinda não há avaliações
- Parts & Design of RPDDocumento18 páginasParts & Design of RPDR KaranAinda não há avaliações
- Raja Nigantu IntroductionDocumento8 páginasRaja Nigantu IntroductionMedico PassAinda não há avaliações
- UKA: When Would I Do It?Documento35 páginasUKA: When Would I Do It?neareastspineAinda não há avaliações
- Periodontal InstrumentsDocumento10 páginasPeriodontal Instrumentsmanishpankaj123100% (1)
- 2019 Fall RNSG 2263 Clinical Mental Health CIDDocumento102 páginas2019 Fall RNSG 2263 Clinical Mental Health CIDadam50% (2)
- Teratogenic ItyDocumento8 páginasTeratogenic ItyValentin IanaAinda não há avaliações
- QC1 Prelims 2019 HandoutsDocumento202 páginasQC1 Prelims 2019 HandoutsFrances Salud40% (5)
- 1358453842.3856hematology Question BankDocumento182 páginas1358453842.3856hematology Question BankKay BristolAinda não há avaliações
- Asymptomatic HyperuricemiaDocumento46 páginasAsymptomatic HyperuricemiaDivya Shree100% (1)
- Tinnitus Today December 1996 Vol 21, No 4Documento31 páginasTinnitus Today December 1996 Vol 21, No 4American Tinnitus AssociationAinda não há avaliações
- ThesisDocumento140 páginasThesisPrem LathaAinda não há avaliações
- Imperforate Anus PDFDocumento2 páginasImperforate Anus PDFGlyneth FranciaAinda não há avaliações
- Case Study On SyphillisDocumento18 páginasCase Study On Syphillisdia_pee100% (1)
- Heart Attack & Drinking Warm WaterDocumento1 páginaHeart Attack & Drinking Warm Waterjoshua_sx180% (5)
- CystosDocumento1 páginaCystosgeorgeloto12Ainda não há avaliações
- 95 Formulation and Evaluation of Diclofenac Sodium Gel by Using Natural PolymerDocumento3 páginas95 Formulation and Evaluation of Diclofenac Sodium Gel by Using Natural PolymerJulian Kayne100% (1)
- TheraSuit BrochureDocumento8 páginasTheraSuit BrochureMhmd IrakyAinda não há avaliações
- Spray Bandage Strategy in Topical Drug DeliveryDocumento9 páginasSpray Bandage Strategy in Topical Drug DeliveryUday BaruahAinda não há avaliações
- Siemens Mri Magnetom Mreadings Prostate PDFDocumento100 páginasSiemens Mri Magnetom Mreadings Prostate PDFnanaa02Ainda não há avaliações
- Current & Future Status of Herbal MedicinesDocumento4 páginasCurrent & Future Status of Herbal MedicinesimmchrAinda não há avaliações
- Fitzgerald AnnInternMed 1999 130 70 Curiosity PDFDocumento3 páginasFitzgerald AnnInternMed 1999 130 70 Curiosity PDFPaulinaAinda não há avaliações
- Raw Materials & Purification - NitrogenDocumento9 páginasRaw Materials & Purification - Nitrogensexyrusty0% (1)
- PNS - Bafs 48-2022 - PNS Veterinary Drug Residues in Food - Product Standard - Maximum Residue Limit (MRL)Documento55 páginasPNS - Bafs 48-2022 - PNS Veterinary Drug Residues in Food - Product Standard - Maximum Residue Limit (MRL)Johana Pinagayao AngkadAinda não há avaliações
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Documento14 páginasNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- Jurnal Beban KerjaDocumento9 páginasJurnal Beban KerjaIsmun SiregarAinda não há avaliações
- 101 Storie ZenDocumento16 páginas101 Storie ZendbrandAinda não há avaliações
- Quantitative Analysis of The Lifting Effect Of.10Documento12 páginasQuantitative Analysis of The Lifting Effect Of.10Arcelino FariasAinda não há avaliações