Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- List of Chemical: FR-PT-GAIN-EMS-21-01Documento2 páginasList of Chemical: FR-PT-GAIN-EMS-21-01henyAinda não há avaliações
- Fundamentals of Pharmacognosy and Phytotherapy 3Rd Edition Heinrich Full ChapterDocumento51 páginasFundamentals of Pharmacognosy and Phytotherapy 3Rd Edition Heinrich Full Chapterbetty.tavares510100% (11)
- Wushu: HerbalismDocumento10 páginasWushu: HerbalismQualia_Ainda não há avaliações
- Oncology Hematology Consultants of South Eastern OhioDocumento3 páginasOncology Hematology Consultants of South Eastern OhioJames LindonAinda não há avaliações
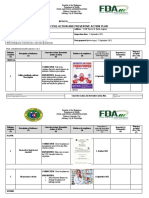
- Capa Plan FormatDocumento4 páginasCapa Plan FormatJERSEY ANN MARIE V. MACALINCAGAinda não há avaliações
- Hypolipidemic Activity of Caralluma Adscendens On Triton and Methimazole Induced Hyperlipidemic RatsDocumento4 páginasHypolipidemic Activity of Caralluma Adscendens On Triton and Methimazole Induced Hyperlipidemic RatsمحمدأميندماجAinda não há avaliações
- Contributory Medical Attendance Rules - BELDocumento64 páginasContributory Medical Attendance Rules - BELVeda PrakashAinda não há avaliações
- Rosemary ExtractDocumento4 páginasRosemary ExtractDr. Syed Khalid HasanAinda não há avaliações
- Prescription-Non Prescription Products: Hitanxi Vyas (19-35) Paridhi Trivedi (19-33) Pharm D 3 YearDocumento19 páginasPrescription-Non Prescription Products: Hitanxi Vyas (19-35) Paridhi Trivedi (19-33) Pharm D 3 Year19-28 Manan PopatAinda não há avaliações
- Oral Pharmacology - For The Dental HygienistDocumento358 páginasOral Pharmacology - For The Dental HygienistIvan GeorgievAinda não há avaliações
- Recommandations Anticoagulante 2015 court-ENDocumento17 páginasRecommandations Anticoagulante 2015 court-ENcatalin petreAinda não há avaliações
- At The Pharmacy Conversations Fun Activities Games Reading Comprehension Exercis - 28726Documento6 páginasAt The Pharmacy Conversations Fun Activities Games Reading Comprehension Exercis - 28726Pablo Meza0% (1)
- M.Pharmacy PCI Syllabus (Pharmaceutical Analysis & Quality Assurance)Documento34 páginasM.Pharmacy PCI Syllabus (Pharmaceutical Analysis & Quality Assurance)PeramharshaAinda não há avaliações
- Anti-Inflammatory Antiarthritis and Related AgentsDocumento10 páginasAnti-Inflammatory Antiarthritis and Related AgentsJustine Vens G. AgustinAinda não há avaliações
- 2008-09-Inhib Prot ĆRPDocumento27 páginas2008-09-Inhib Prot ĆRPapi-3814389Ainda não há avaliações
- LysoformDocumento4 páginasLysoformRajiv SinghAinda não há avaliações
- Daftar Harga Tiap PBFDocumento5 páginasDaftar Harga Tiap PBFjuniAinda não há avaliações
- Cinética de Deshidratación Osmótica Del Albaricoque Con Solución de Sacarosa.Documento9 páginasCinética de Deshidratación Osmótica Del Albaricoque Con Solución de Sacarosa.Alejandra OrtegaAinda não há avaliações
- Risk Assessment Example 1Documento3 páginasRisk Assessment Example 1miptahul100% (3)
- Cefpodoxime 200 Tab New 1Documento25 páginasCefpodoxime 200 Tab New 1Gurdev SinghAinda não há avaliações
- Stock Farmacia 28-02-2014Documento20 páginasStock Farmacia 28-02-2014Carlos Manuel Sanchez SanchezAinda não há avaliações
- Presented By:-Group 8 Alok Somani Ruchi Agrawal Madhuri Kabade Kamini Varma Vidit GuptaDocumento14 páginasPresented By:-Group 8 Alok Somani Ruchi Agrawal Madhuri Kabade Kamini Varma Vidit GuptaJuBin DeliwalaAinda não há avaliações
- Chemistry in Everyday LifeDocumento4 páginasChemistry in Everyday LifeAbhisek PandaAinda não há avaliações
- Valvulas Diafragma Asepticas BPEDocumento104 páginasValvulas Diafragma Asepticas BPEHumberto GonzálezAinda não há avaliações
- David KaniosDocumento28 páginasDavid KaniosJoko RinantoAinda não há avaliações
- PSMB Area 4Documento133 páginasPSMB Area 4Princess Rose GamboaAinda não há avaliações
- Bioavailability Studies Submitted in Ndas or Inds - General ConsiderationsDocumento30 páginasBioavailability Studies Submitted in Ndas or Inds - General ConsiderationsSrinivas Reddy MaramAinda não há avaliações
- Reflective WritingDocumento2 páginasReflective WritingJoyce VillanuevaAinda não há avaliações
- Gland Pharma AR Final 19 20Documento108 páginasGland Pharma AR Final 19 20TotmolAinda não há avaliações
- Appl Sartobind Virus Purification Removal SL-4038-e06012Documento4 páginasAppl Sartobind Virus Purification Removal SL-4038-e06012Yaser WazirAinda não há avaliações