Você também pode gostar
- Bowen Family TheoryDocumento320 páginasBowen Family Theorytonifieraru100% (14)
- 1000 Calorie ChallengesDocumento25 páginas1000 Calorie ChallengesFrancesco Iavarone100% (3)
- Braden ScaleDocumento2 páginasBraden ScaleAJ Tuban CompelioAinda não há avaliações
- Questions DRDocumento8 páginasQuestions DRRosalie Valdez EspirituAinda não há avaliações
- Science and Practice of Pressure Ulcer ManagementDocumento213 páginasScience and Practice of Pressure Ulcer ManagementRoy GoldenAinda não há avaliações
- Worksheet For Nervous Systems-KeyDocumento5 páginasWorksheet For Nervous Systems-KeyNazarine Torres100% (2)
- Malaria Lesson Plan 1Documento3 páginasMalaria Lesson Plan 1Jayshree ParmarAinda não há avaliações
- Chapter 32 - Stop-Controlled Intersections Supp - 600Documento74 páginasChapter 32 - Stop-Controlled Intersections Supp - 600Ana María Lira CastroAinda não há avaliações
- Passport XG Service ManualDocumento544 páginasPassport XG Service ManualThatch50% (2)
- BIA at Bedside Review Mulasi NCP2015Documento14 páginasBIA at Bedside Review Mulasi NCP2015julianapandiniAinda não há avaliações
- Evaluation of Muscle and Fat Loss As Diagnostic Criteria For MalnutritionDocumento10 páginasEvaluation of Muscle and Fat Loss As Diagnostic Criteria For MalnutritionOctavianus KevinAinda não há avaliações
- Pediatric Malnutrition: Putting The New Definition and Standards Into PracticeDocumento16 páginasPediatric Malnutrition: Putting The New Definition and Standards Into PracticeEugenia BocaAinda não há avaliações
- Nutrition in Clinical PracticeDocumento13 páginasNutrition in Clinical PracticeSCPAinda não há avaliações
- Pediatric Malnutrition Putting The New Definition and Standards Into PracticeDocumento17 páginasPediatric Malnutrition Putting The New Definition and Standards Into PracticeOctavianus KevinAinda não há avaliações
- Dietary Considerations For The Sick and Hospitalized PatientsDocumento7 páginasDietary Considerations For The Sick and Hospitalized Patientsgaurav sharmaAinda não há avaliações
- Use of 3 Tools To Assess Nutrition Risk in The Intensive Care UnitDocumento6 páginasUse of 3 Tools To Assess Nutrition Risk in The Intensive Care UnitnanitaAinda não há avaliações
- Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & LoveDocumento12 páginasBailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & LoveSaifianAinda não há avaliações
- Jurnal 3 KMB 2Documento14 páginasJurnal 3 KMB 2Devi AmbarwatiAinda não há avaliações
- Utilization of Nutrition-Focused Physical AssessmentDocumento9 páginasUtilization of Nutrition-Focused Physical AssessmentRocio SantelizAinda não há avaliações
- 336.nut in Clin Prac - 2017 - Dickerson - Protein and Calorie Requirements Associated With The Presence of ObesityDocumento8 páginas336.nut in Clin Prac - 2017 - Dickerson - Protein and Calorie Requirements Associated With The Presence of ObesitytereAinda não há avaliações
- Protein and Calorie Requirements Associated With The Presence of ObesityDocumento8 páginasProtein and Calorie Requirements Associated With The Presence of ObesityRaman ChaudharyAinda não há avaliações
- JMedNutrNutraceut2277-5417572 150255Documento7 páginasJMedNutrNutraceut2277-5417572 150255jufranAinda não há avaliações
- Nutritional Support NotesDocumento14 páginasNutritional Support NotesAudrie Allyson GabalesAinda não há avaliações
- Nutrition in Intensive Care in Adults Review of The Literature and Development of Evidence Based Feeding ProtocolsDocumento12 páginasNutrition in Intensive Care in Adults Review of The Literature and Development of Evidence Based Feeding ProtocolsnwghnutritionistAinda não há avaliações
- NFPA Micronutrient NCP 15pdfDocumento10 páginasNFPA Micronutrient NCP 15pdfMorellia zapataAinda não há avaliações
- Rol Del To PDFDocumento4 páginasRol Del To PDFMaria Laura SoriaAinda não há avaliações
- Post-ICU Nutrition The Neglected Side of Metabolic SupportDocumento3 páginasPost-ICU Nutrition The Neglected Side of Metabolic SupportHubert PastasAinda não há avaliações
- Critical Ill PDFDocumento5 páginasCritical Ill PDFAnish H DaveAinda não há avaliações
- Enteral FormulationsDocumento14 páginasEnteral Formulationsingrit tatiana martinez laraAinda não há avaliações
- FOS JournalDocumento14 páginasFOS JournalXII - G - 09 - Jessica WijayaAinda não há avaliações
- ACG Clinical Guideline: Nutrition Therapy in The Adult Hospitalized PatientDocumento20 páginasACG Clinical Guideline: Nutrition Therapy in The Adult Hospitalized PatientLetícia MachadoAinda não há avaliações
- GlikogenDocumento5 páginasGlikogenliaAinda não há avaliações
- Aspen Guidelines SurgicalDocumento10 páginasAspen Guidelines SurgicalJeshuanna DelgadoAinda não há avaliações
- ESPEN Guidelines On Parenteral Nutrition Surgery 2006Documento9 páginasESPEN Guidelines On Parenteral Nutrition Surgery 2006Jorge OsorioAinda não há avaliações
- Medicamentos e AlimentosDocumento8 páginasMedicamentos e AlimentosPhilipe VieiraAinda não há avaliações
- Dietary Treatment of Intractable Epilepsy: Review ArticleDocumento11 páginasDietary Treatment of Intractable Epilepsy: Review ArticleArdiya OktamaAinda não há avaliações
- Culinary Medicine: Paving The Way To Health Through Our ForksDocumento3 páginasCulinary Medicine: Paving The Way To Health Through Our ForksJyothi MallyaAinda não há avaliações
- A Guide For Optimizing Nutritional Support in The Critically Ill ChildDocumento7 páginasA Guide For Optimizing Nutritional Support in The Critically Ill ChildNeny Reni DwulandariAinda não há avaliações
- Parenteral Nutrition: Key ConceptsDocumento19 páginasParenteral Nutrition: Key Conceptsdwinov educationAinda não há avaliações
- 3-In-1vs2-In-1 Multi Chamber Parenteral NutritionDocumento6 páginas3-In-1vs2-In-1 Multi Chamber Parenteral NutritionPatricia DalanAinda não há avaliações
- 2015 Nutrition Managementt of The Postbariatric Surgery PatientDocumento10 páginas2015 Nutrition Managementt of The Postbariatric Surgery PatientykommAinda não há avaliações
- Impact of A Computerized InforDocumento10 páginasImpact of A Computerized Inforsaya amirazAinda não há avaliações
- MadsenArticle July 06Documento16 páginasMadsenArticle July 06Kouba MarciminiAinda não há avaliações
- Nutrition Priorities in Obese Critically Ill.10Documento11 páginasNutrition Priorities in Obese Critically Ill.10Iván OsunaAinda não há avaliações
- Nutrition and Wound Healing: Ryan Katz, MD Adrian Barbul, MD, FACSDocumento9 páginasNutrition and Wound Healing: Ryan Katz, MD Adrian Barbul, MD, FACSAlinaAinda não há avaliações
- J Parenter Enteral Nutr - 2013 - Choban - A S P E N Clinical GuidelinesDocumento31 páginasJ Parenter Enteral Nutr - 2013 - Choban - A S P E N Clinical Guidelinescarlos enriqueAinda não há avaliações
- Unexpected Physiological Limit in Comparison To More Youthful Individuals of Clinical PreliminariesDocumento2 páginasUnexpected Physiological Limit in Comparison To More Youthful Individuals of Clinical PreliminariesHas SimAinda não há avaliações
- Skipper 1992Documento4 páginasSkipper 1992Federico CilloAinda não há avaliações
- 1 s2.0 S2405457722000432 MainDocumento7 páginas1 s2.0 S2405457722000432 MainjvracuyaAinda não há avaliações
- Nutri Final 1Documento4 páginasNutri Final 1cajeshannahabigaelAinda não há avaliações
- Nutrition - Parenteral 2Documento16 páginasNutrition - Parenteral 2Guillaume michiganAinda não há avaliações
- Macronutrientes y EnergiaDocumento8 páginasMacronutrientes y Energianathalie mercadoAinda não há avaliações
- Risk For Imbalanced NutritionDocumento3 páginasRisk For Imbalanced Nutritionaudreyann.acobAinda não há avaliações
- 2011 Corrigan - Nutrition in Stroke PatientsDocumento11 páginas2011 Corrigan - Nutrition in Stroke PatientsAmy100% (1)
- Dietary Recommendation For Fasting DaysDocumento6 páginasDietary Recommendation For Fasting DaysChicaiza Tituana JhonnAinda não há avaliações
- Hypocaloric, High-Protein Nutrition Therapy For Critically Ill Patients With ObesityDocumento7 páginasHypocaloric, High-Protein Nutrition Therapy For Critically Ill Patients With ObesityStacey WoodsAinda não há avaliações
- Mindanao State University: Nursing Care Plan For Cancer DiseasesDocumento11 páginasMindanao State University: Nursing Care Plan For Cancer DiseasesAngelica Charisse BuliganAinda não há avaliações
- Pearce, 2002Documento7 páginasPearce, 2002Citta ArastiAinda não há avaliações
- Assessment Nursing Diagnosis Rationale Planning Implementation Rationale EvaluationDocumento2 páginasAssessment Nursing Diagnosis Rationale Planning Implementation Rationale EvaluationHsintan HsuAinda não há avaliações
- Enteral and Parenteral Applications of Ketogenic Diet TherapyDocumento8 páginasEnteral and Parenteral Applications of Ketogenic Diet TherapyFauzan MuhammadAinda não há avaliações
- J Parenter Enteral Nutr - 2017 - Mehta - Guidelines For The Provision and Assessment of Nutrition Support Therapy in TheDocumento37 páginasJ Parenter Enteral Nutr - 2017 - Mehta - Guidelines For The Provision and Assessment of Nutrition Support Therapy in TheZ. Raquel García OsornoAinda não há avaliações
- Should Handgrip Strength Be Considered When ChoosingDocumento6 páginasShould Handgrip Strength Be Considered When ChoosingJuciara MouraAinda não há avaliações
- Acheson Et Al (1980)Documento8 páginasAcheson Et Al (1980)Callum BromleyAinda não há avaliações
- Rodriguez 2011, Nutrition in Burns Galveston ContributionsDocumento11 páginasRodriguez 2011, Nutrition in Burns Galveston Contributionsdiana perezAinda não há avaliações
- Aarc Copd - Nutritional Assessment and GuidelinesDocumento51 páginasAarc Copd - Nutritional Assessment and GuidelinesRJAY VINCENT BUENAFEAinda não há avaliações
- Nutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansDocumento7 páginasNutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansangiolikkiaAinda não há avaliações
- Letters: Role of Dietitians in Reducing Malnutrition in HospitalDocumento1 páginaLetters: Role of Dietitians in Reducing Malnutrition in HospitalShanty OktaviaAinda não há avaliações
- Choban 2013Documento32 páginasChoban 2013Constanza CraAinda não há avaliações
- Nutrition: A Handbook for NursesNo EverandNutrition: A Handbook for NursesCarolyn BestAinda não há avaliações
- Jurnal Remifentanyl For Pain LaborDocumento11 páginasJurnal Remifentanyl For Pain LaborAshadi CahyadiAinda não há avaliações
- The Tragedy of Schizophrenia Without PsychotherapyDocumento30 páginasThe Tragedy of Schizophrenia Without PsychotherapyRachel AHAinda não há avaliações
- عملیات شفاء امراض Amliyat Shifa Amraz 0091-33-23607502 - DIL KE AMRAZ KA RUHANI ELAJ (Spiritual Treatment of Heart Diseases)Documento4 páginasعملیات شفاء امراض Amliyat Shifa Amraz 0091-33-23607502 - DIL KE AMRAZ KA RUHANI ELAJ (Spiritual Treatment of Heart Diseases)msmpaki@yahoo.comAinda não há avaliações
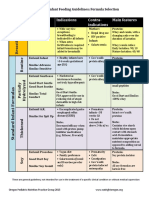
- Formula Selection OPNPGDocumento2 páginasFormula Selection OPNPGRina PratiwiAinda não há avaliações
- Laboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Documento3 páginasLaboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Ramesh KumarAinda não há avaliações
- Pop Q ReferenceDocumento18 páginasPop Q ReferenceEdwin KurniawanAinda não há avaliações
- FD PDFDocumento580 páginasFD PDFAinul LuthfiAinda não há avaliações
- Kainan University ApplicationDocumento25 páginasKainan University ApplicationGeraldine RiveraAinda não há avaliações
- CPR and Aed: Quiz #2 ResultsDocumento2 páginasCPR and Aed: Quiz #2 ResultsNathan WhiteAinda não há avaliações
- An Analytical Study of Euthanasia in India With - Rucha Kulkarni PDFDocumento150 páginasAn Analytical Study of Euthanasia in India With - Rucha Kulkarni PDFDazzler AshishAinda não há avaliações
- Amy WebDocumento62 páginasAmy WebAnotherAnonymomAinda não há avaliações
- Post Natal ExercisesDocumento7 páginasPost Natal ExercisesEvie Dolpin BlueAinda não há avaliações
- Ast (Sgot) ColorDocumento2 páginasAst (Sgot) ColorShribagla MukhiAinda não há avaliações
- Advanced Cardiovascular Life Support (ACLS)Documento27 páginasAdvanced Cardiovascular Life Support (ACLS)Sara Ali100% (3)
- Animal Welfare Board of India v. A Nagaraja & Ors PDFDocumento117 páginasAnimal Welfare Board of India v. A Nagaraja & Ors PDFBar & Bench100% (1)
- Mechanical Ventilation 2015Documento18 páginasMechanical Ventilation 2015Nauman GilaniAinda não há avaliações
- Immunology Mcqs-I (Gate Helpline)Documento5 páginasImmunology Mcqs-I (Gate Helpline)Santhosh KalashAinda não há avaliações
- Tdah 20Documento14 páginasTdah 20Roberto Alexis Molina CampuzanoAinda não há avaliações
- Myomodulation With Facial Fillers A ComprehensiveDocumento13 páginasMyomodulation With Facial Fillers A ComprehensiveThiago MouraAinda não há avaliações
- Mayur - 01Documento2 páginasMayur - 01mukesh jambukiyaAinda não há avaliações
- Perbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorDocumento7 páginasPerbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorAAK DHGRiski MaulanaAinda não há avaliações