Você também pode gostar
- Guía práctica para técnico superior de laboratorio de diagnóstico clínico y biomédicoNo EverandGuía práctica para técnico superior de laboratorio de diagnóstico clínico y biomédicoNota: 4.5 de 5 estrelas4.5/5 (10)
- Combate de AngamosDocumento3 páginasCombate de AngamosBruno Aurelio Huallan Padilla83% (6)
- Principios básicos de patología para fisioterapia: Volumen INo EverandPrincipios básicos de patología para fisioterapia: Volumen IAinda não há avaliações
- Clase 6. Contactos Interoclusales (Reparado)Documento6 páginasClase 6. Contactos Interoclusales (Reparado)Bruno Aurelio Huallan Padilla100% (1)
- LIBTRAS008Documento20 páginasLIBTRAS008Beatriz Luque GarridoAinda não há avaliações
- PsionicaDocumento41 páginasPsionicaCarlos GS100% (5)
- Familia PichilínDocumento13 páginasFamilia Pichilínyulansi17% (6)
- Clase 5. Desoclusión y Guía AnteriorDocumento7 páginasClase 5. Desoclusión y Guía AnteriorBruno Aurelio Huallan Padilla50% (2)
- Carta Descriptiva "Respuesta Inmune" 20-1Documento19 páginasCarta Descriptiva "Respuesta Inmune" 20-1Ruth Cobo RosalesAinda não há avaliações
- Comprension de Lectura El Valor Nutritivo de Los AlimentosDocumento4 páginasComprension de Lectura El Valor Nutritivo de Los AlimentosLeslie Merino Méndez100% (10)
- Laboratorio de Biologia y Genetica MolecularDocumento15 páginasLaboratorio de Biologia y Genetica MolecularAdri Pamelita TorresAinda não há avaliações
- 1 Derecho Notarial y RegistralDocumento38 páginas1 Derecho Notarial y Registralreyna burboa100% (2)
- Guía Práctica PDFDocumento52 páginasGuía Práctica PDFLuis Sierra100% (1)
- TALLER 1 BC 2024Documento4 páginasTALLER 1 BC 2024alesromy2004Ainda não há avaliações
- Taller 1 Parte A y Parte BDocumento8 páginasTaller 1 Parte A y Parte BMilagros Belen GilAinda não há avaliações
- Taller 4 2020Documento5 páginasTaller 4 2020JOEL COLORADOAinda não há avaliações
- Taller 2 BC 2024Documento5 páginasTaller 2 BC 2024Gastón LlampaAinda não há avaliações
- Taller 2 Biología CelularDocumento5 páginasTaller 2 Biología Celularjules BianchiAinda não há avaliações
- Taller 6 Biología Celular 2020Documento7 páginasTaller 6 Biología Celular 2020JOEL COLORADOAinda não há avaliações
- Técnicas de biología molecular para detección de ácidos nucleicosDocumento15 páginasTécnicas de biología molecular para detección de ácidos nucleicosDaya AtienciaAinda não há avaliações
- Manual Laboratorio Biología Celular Ii, 2018 Oficial PDFDocumento75 páginasManual Laboratorio Biología Celular Ii, 2018 Oficial PDFByron PocasangreAinda não há avaliações
- Presentación Tema 1. BMCDocumento43 páginasPresentación Tema 1. BMCnereavazquez16Ainda não há avaliações
- Universidad Mariano Gálvez Facultad de Ciencias Médicas y de La SaludDocumento70 páginasUniversidad Mariano Gálvez Facultad de Ciencias Médicas y de La SaludJESUS OCTAVIO GUTIERREZAinda não há avaliações
- Taller 1 Genetica 2023Documento5 páginasTaller 1 Genetica 2023Mercedes EscobarAinda não há avaliações
- 30-INMUTECNOLOGIASDocumento6 páginas30-INMUTECNOLOGIASFabricio CascoAinda não há avaliações
- Notas de Clase Semana N°10Documento11 páginasNotas de Clase Semana N°10Miguel OrtegaAinda não há avaliações
- Diagnostico en Biologia MolecularDocumento34 páginasDiagnostico en Biologia MolecularZaidaAinda não há avaliações
- 2007 Manual Metodos Inmunologicos Completo Web PDFDocumento139 páginas2007 Manual Metodos Inmunologicos Completo Web PDFLiliana LinoAinda não há avaliações
- Cbo Tesis Doctoral PDFDocumento101 páginasCbo Tesis Doctoral PDFJesus Bautisto Huichi JaraAinda não há avaliações
- Cbo Tesis Doctoral PDFDocumento203 páginasCbo Tesis Doctoral PDFOlenka Cerpa PlasenciaAinda não há avaliações
- Tesis - Muñoz Jiménez, AlejandroDocumento298 páginasTesis - Muñoz Jiménez, Alejandromnica1977Ainda não há avaliações
- Anatomía Patológica: Diagnósticos y Procesos LesivosDocumento64 páginasAnatomía Patológica: Diagnósticos y Procesos LesivosNayaraAinda não há avaliações
- Manual F y BF IDocumento37 páginasManual F y BF ISandra Anahí Rubio TorresAinda não há avaliações
- Guia 5 2021 - Laboratorio y Miscelaneas - InddDocumento26 páginasGuia 5 2021 - Laboratorio y Miscelaneas - InddMariano AlbertiAinda não há avaliações
- Biologia Molecular en Micologia MedicaDocumento4 páginasBiologia Molecular en Micologia MedicaSara BarcenasAinda não há avaliações
- Review Biologia Molecular y CelularDocumento17 páginasReview Biologia Molecular y CelularLuis Argumedo MéndezAinda não há avaliações
- Procesamiento en PatologíaDocumento6 páginasProcesamiento en PatologíaSebastian PinillaAinda não há avaliações
- GUIA 4 - Inmunofluorescencia y Detección de VirusDocumento9 páginasGUIA 4 - Inmunofluorescencia y Detección de VirusMaria Fernanda Ortiz AndradeAinda não há avaliações
- Técnicas de Diagnóstico Con Biología MolecularDocumento6 páginasTécnicas de Diagnóstico Con Biología MolecularNuviaAinda não há avaliações
- Seimc Procedimientomicrobiologia18Documento68 páginasSeimc Procedimientomicrobiologia18dcrosiwiAinda não há avaliações
- Guía de laboratorio virtual sobre mitosisDocumento5 páginasGuía de laboratorio virtual sobre mitosisCamilo Cortina AlfaroAinda não há avaliações
- TP1 2022Documento3 páginasTP1 2022Vir SAinda não há avaliações
- Seminario 5 Tecnicas I BC 2020 Fmed UBA (PDF - Io)Documento48 páginasSeminario 5 Tecnicas I BC 2020 Fmed UBA (PDF - Io)Emilio Sáez ValdésAinda não há avaliações
- Taller 2 BC Parte A y BDocumento4 páginasTaller 2 BC Parte A y BLola RodriguezAinda não há avaliações
- Tema 1Documento24 páginasTema 1NEREA LAGUNA SERRANOAinda não há avaliações
- Preguntas para Analizar - Unidad 3 - Genética - Tarea 4.Documento3 páginasPreguntas para Analizar - Unidad 3 - Genética - Tarea 4.Sofia MejiaAinda não há avaliações
- Manual Homologado de Inmuno-RevisadoDocumento40 páginasManual Homologado de Inmuno-RevisadoCortesgamez MalinalliAinda não há avaliações
- Laboratorios Grupos C y D 2015 PDFDocumento26 páginasLaboratorios Grupos C y D 2015 PDFGabriela GualimAinda não há avaliações
- P2 - Técnicas en Biología MolecularDocumento5 páginasP2 - Técnicas en Biología MolecularMARIANA YEPES MEJIAAinda não há avaliações
- Tecnicas Especiales en Patologia Ues 22Documento75 páginasTecnicas Especiales en Patologia Ues 22Bruno Arnaldo Flores VenegasAinda não há avaliações
- Manual Homologado de Inmuno - 2022 - Revisión Otoño 22Documento40 páginasManual Homologado de Inmuno - 2022 - Revisión Otoño 22XPcrasher 96Ainda não há avaliações
- Técnicas del PCRDocumento15 páginasTécnicas del PCRYosue AraúzAinda não há avaliações
- MD2012Documento5 páginasMD2012Alexander GangAinda não há avaliações
- Técnias Detección de Antígeno PDFDocumento62 páginasTécnias Detección de Antígeno PDFjaverachAinda não há avaliações
- MANUALDocumento62 páginasMANUALMayra Janette Jane SkłodowskaAinda não há avaliações
- Biologia Celular y GeneticaDocumento4 páginasBiologia Celular y GeneticaandresAinda não há avaliações
- Manual de Practica de InmunoDocumento73 páginasManual de Practica de InmunoDENNIS RUBEN SOLANO CASTAÑEDAAinda não há avaliações
- Silabo Biol Mol 2019 CDocumento7 páginasSilabo Biol Mol 2019 CTifanny Cuellar RamosAinda não há avaliações
- Apuntes de Patología GeneralDocumento11 páginasApuntes de Patología GeneralRaul Arciniega EscorciaAinda não há avaliações
- Practica 3 biologia celular.docx 45 (1) (2).docx 345 (1)Documento14 páginasPractica 3 biologia celular.docx 45 (1) (2).docx 345 (1)DAVID ALEXANDER DE LA CRUZ ALCIVARAinda não há avaliações
- TD Vera Rivero Francisco MiguelDocumento228 páginasTD Vera Rivero Francisco MiguelIsabella María GantivarAinda não há avaliações
- Imagenes PatológicasDocumento7 páginasImagenes PatológicasPau FlurscheimAinda não há avaliações
- Procedimeintos en Microbiologia Clinica MolecularDocumento68 páginasProcedimeintos en Microbiologia Clinica MolecularCésar Omar Gálvez GonzálezAinda não há avaliações
- Herrero Monica VivianaDocumento128 páginasHerrero Monica Vivianapayo gcAinda não há avaliações
- PRÁCTICA Nº01 Diagnóstico Directo de Leishmania SPPDocumento7 páginasPRÁCTICA Nº01 Diagnóstico Directo de Leishmania SPPAli SamanthaAinda não há avaliações
- Biología Molecular y Celular: Una guía introductoria para aprender Biología Celular y MolecularNo EverandBiología Molecular y Celular: Una guía introductoria para aprender Biología Celular y MolecularAinda não há avaliações
- Material Microscopia y TecnicasDocumento8 páginasMaterial Microscopia y TecnicasBruno Aurelio Huallan PadillaAinda não há avaliações
- Clase 2 Impresiones y ModelosDocumento4 páginasClase 2 Impresiones y ModelosBrunoAinda não há avaliações
- CLASE 2 Corrección de ModelosDocumento2 páginasCLASE 2 Corrección de ModelosBruno Aurelio Huallan PadillaAinda não há avaliações
- Clase 3. Articuladores, Inducción y MontajeDocumento6 páginasClase 3. Articuladores, Inducción y MontajeBrunoAinda não há avaliações
- Clase 2 OCLUSIÓN-ATM-MOV - MANDIBULARESDocumento5 páginasClase 2 OCLUSIÓN-ATM-MOV - MANDIBULARESBruno Aurelio Huallan PadillaAinda não há avaliações
- Clase 7. Diagnóstico Sobre ModelosDocumento5 páginasClase 7. Diagnóstico Sobre ModelosBruno Aurelio Huallan PadillaAinda não há avaliações
- PULMONESDocumento12 páginasPULMONESMarianne MarksAinda não há avaliações
- CLASE 4 Desoclusión, ATM y Alineación TridimensionalDocumento4 páginasCLASE 4 Desoclusión, ATM y Alineación TridimensionalBruno Aurelio Huallan Padilla100% (1)
- Clase 2 Impresiones y ModelosDocumento4 páginasClase 2 Impresiones y ModelosBrunoAinda não há avaliações
- Clase 3. Articuladores, Inducción y MontajeDocumento6 páginasClase 3. Articuladores, Inducción y MontajeBrunoAinda não há avaliações
- Adición y Sustracción de MonomiosDocumento2 páginasAdición y Sustracción de MonomiosPedro Garcia68% (19)
- Resumen 1er Parcial HistoriaDocumento4 páginasResumen 1er Parcial HistoriaBruno Aurelio Huallan PadillaAinda não há avaliações
- Historias para NiñosDocumento5 páginasHistorias para NiñosMarco GabrielAinda não há avaliações
- AngulosDocumento2 páginasAngulosBruno Aurelio Huallan Padilla0% (2)
- El Gigante ClementínDocumento1 páginaEl Gigante ClementínMatthew Maynard100% (2)
- Memoria Ram WikiDocumento1 páginaMemoria Ram WikiBruno Aurelio Huallan PadillaAinda não há avaliações
- Envio de La LibertadDocumento1 páginaEnvio de La LibertadBruno Aurelio Huallan PadillaAinda não há avaliações
- Celula Bacteriana PDFDocumento86 páginasCelula Bacteriana PDFBruno Aurelio Huallan PadillaAinda não há avaliações
- Florencia de MoraDocumento1 páginaFlorencia de MoraBruno Aurelio Huallan Padilla100% (1)
- Matematica 51 - Guia 4 Funciones Exponenciales y LogaritmicasDocumento88 páginasMatematica 51 - Guia 4 Funciones Exponenciales y LogaritmicasTwiggy ShapiamaAinda não há avaliações
- Vias de ConduccionDocumento90 páginasVias de ConduccionEmiliano Salas PortaAinda não há avaliações
- Dieta de FutbolistaDocumento1 páginaDieta de FutbolistaBruno Aurelio Huallan PadillaAinda não há avaliações
- Ingles HowDocumento2 páginasIngles HowBruno Aurelio Huallan PadillaAinda não há avaliações
- Matematica 51 - Guía 6 - IntegralesDocumento41 páginasMatematica 51 - Guía 6 - IntegralesTwiggy ShapiamaAinda não há avaliações
- Drenaje de CabezaDocumento12 páginasDrenaje de CabezaBruno Aurelio Huallan PadillaAinda não há avaliações
- Secado RapidoDocumento2 páginasSecado RapidoJobanny Uc RosadoAinda não há avaliações
- Corte 7 Hector Lopez Etapa 5Documento2 páginasCorte 7 Hector Lopez Etapa 5camila corredorAinda não há avaliações
- Memorias Sesión # 2 Emprendelo Mayo 6 de 2021Documento131 páginasMemorias Sesión # 2 Emprendelo Mayo 6 de 2021ricardo ladinoAinda não há avaliações
- SRAMDocumento12 páginasSRAMque buenoAinda não há avaliações
- Hechos Como Fundamentos JurídicosDocumento2 páginasHechos Como Fundamentos JurídicosTelvy Elizabeth Chamaya GuevaraAinda não há avaliações
- Biografía Del Río SeturmaDocumento12 páginasBiografía Del Río SeturmaJorge Luis Gonzalez BermudezAinda não há avaliações
- Historia de La AstronomiaDocumento6 páginasHistoria de La AstronomiaNeidy Rios AguileraAinda não há avaliações
- Modos de VMDocumento7 páginasModos de VMLizbeth CMAinda não há avaliações
- GáaaaaaaaaDocumento14 páginasGáaaaaaaaaMaycol Sánchez EspinozaAinda não há avaliações
- Power Cuello - Segunda ParteDocumento57 páginasPower Cuello - Segunda ParteMauro MolinaAinda não há avaliações
- Pag 64 Crucigrama 1Documento1 páginaPag 64 Crucigrama 1Diego CadenasAinda não há avaliações
- Identificacion Puntos Criticos SI... +Documento3 páginasIdentificacion Puntos Criticos SI... +cristian felipe ortega ceronAinda não há avaliações
- Técnicas - Trabajo de EquipoDocumento17 páginasTécnicas - Trabajo de EquipoAstrip100% (15)
- Causa Báez PDFDocumento167 páginasCausa Báez PDFSerá JusticiaAinda não há avaliações
- Ecografia Recomendaciones. Nov 2020 - CompressedDocumento30 páginasEcografia Recomendaciones. Nov 2020 - CompressedyuyoeightAinda não há avaliações
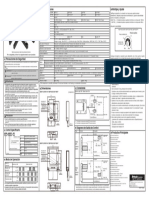
- Autonics Bup Esp ManualDocumento1 páginaAutonics Bup Esp ManualfchumpitazAinda não há avaliações
- Ciclo Menstrual y Desarrollo EmbrionarioDocumento12 páginasCiclo Menstrual y Desarrollo EmbrionarioRodriguez JuanitaAinda não há avaliações
- Masticacion Clinica de NiñoDocumento18 páginasMasticacion Clinica de NiñoBibi MoleAinda não há avaliações
- Lagun-Aro EPSV / Te Asistimos en El ExtranjeroDocumento3 páginasLagun-Aro EPSV / Te Asistimos en El ExtranjeroLagun-AroEPSVAinda não há avaliações
- Enrutamiento de ASPDocumento10 páginasEnrutamiento de ASPjasmanyAinda não há avaliações
- Órgano Judicial Comparación Entre Gobiernos DiapositivasDocumento10 páginasÓrgano Judicial Comparación Entre Gobiernos DiapositivasVanelizRodríguezAinda não há avaliações
- Darling Tatiana Valencia Alzate: 17 OYS 1931620 CC 1023005482Documento1 páginaDarling Tatiana Valencia Alzate: 17 OYS 1931620 CC 1023005482Tatiana Espitia MeloAinda não há avaliações
- Diagrama HierroDocumento8 páginasDiagrama Hierropineda1505Ainda não há avaliações
- Citas VancouverDocumento14 páginasCitas VancouvermaveguitaAinda não há avaliações
- MúsicaDocumento96 páginasMúsicaJose Antonio HernanAinda não há avaliações
- ProcDigImgUNMSMDocumento24 páginasProcDigImgUNMSMDiego Alonso FloresAinda não há avaliações
- Enfermeria TecnicaDocumento1 páginaEnfermeria TecnicaCesar FarroAinda não há avaliações
- TAREA I Música - ERIKAEUGENIDocumento3 páginasTAREA I Música - ERIKAEUGENIErika EugeniAinda não há avaliações