Você também pode gostar
- Full Autopsy Released in Death of Kyler PresnellDocumento9 páginasFull Autopsy Released in Death of Kyler PresnellKrystyna May67% (3)
- The Little Book of Sexual HappinessDocumento40 páginasThe Little Book of Sexual Happinesswolf4853100% (2)
- Textbook of Physiotherapy For Obstetric and Gynecological Conditions MASUD PDFDocumento205 páginasTextbook of Physiotherapy For Obstetric and Gynecological Conditions MASUD PDFAlina Gherman-Haiduc75% (4)
- Urological EmergencyDocumento83 páginasUrological EmergencyAlfred LiAinda não há avaliações
- TuberculosisDocumento42 páginasTuberculosisGilbertoMpakaniyeAinda não há avaliações
- Practical Pediatric Hematology PDFDocumento350 páginasPractical Pediatric Hematology PDFHaris Qurashi100% (2)
- Rubella: Dr.T.V.Rao MDDocumento42 páginasRubella: Dr.T.V.Rao MDtummalapalli venkateswara raoAinda não há avaliações
- CPM7th TB in Infancy and ChildhoodDocumento41 páginasCPM7th TB in Infancy and ChildhoodJackyAinda não há avaliações
- Selectividad Abuseofantibiotics - June2001Documento3 páginasSelectividad Abuseofantibiotics - June2001Penny RivasAinda não há avaliações
- The Pathogenic Basis of Malaria: InsightDocumento7 páginasThe Pathogenic Basis of Malaria: InsightRaena SepryanaAinda não há avaliações
- Mycobacterium General Properties: Mycobacteria Cell Wall StructureDocumento12 páginasMycobacterium General Properties: Mycobacteria Cell Wall StructureAhmed ExaminationAinda não há avaliações
- MycobacteriumDocumento14 páginasMycobacteriumSnowie BalansagAinda não há avaliações
- Acid Fast Bacteria: M. Tuberculosis, M. LepraeDocumento22 páginasAcid Fast Bacteria: M. Tuberculosis, M. LepraeelaAinda não há avaliações
- Chapter IX MycobacteriaDocumento40 páginasChapter IX Mycobacteriayosef awokeAinda não há avaliações
- Immunity Against MycobacteriaDocumento9 páginasImmunity Against MycobacteriadarmariantoAinda não há avaliações
- Tuberculosis Patogeno AdaptableDocumento15 páginasTuberculosis Patogeno AdaptableMisael VegaAinda não há avaliações
- MycobacteriumDocumento9 páginasMycobacteriumمحمد رائد رزاق إسماعيلAinda não há avaliações
- Fimmu 09 02219Documento13 páginasFimmu 09 02219skgs1970Ainda não há avaliações
- Mjhid 6 1 E2014027Documento11 páginasMjhid 6 1 E2014027Son DellAinda não há avaliações
- Tuberculosis: Mechanism and TherapyDocumento6 páginasTuberculosis: Mechanism and TherapyHyeong Ghil ShinAinda não há avaliações
- Mycobacterium Tuberculosis:: 1. Pulmonary Disease 2. Extra-Pulmonary Disseminated DiseaseDocumento3 páginasMycobacterium Tuberculosis:: 1. Pulmonary Disease 2. Extra-Pulmonary Disseminated Diseasesmart_dudeAinda não há avaliações
- Cutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDocumento10 páginasCutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDellAinda não há avaliações
- How Can Immunology Contribute To The Control of Tuberculosis?Documento11 páginasHow Can Immunology Contribute To The Control of Tuberculosis?Parijat BanerjeeAinda não há avaliações
- Tmp2a66 TMPDocumento4 páginasTmp2a66 TMPFrontiersAinda não há avaliações
- 2611 7525 1 SMDocumento12 páginas2611 7525 1 SMAliza Dewi FortuaAinda não há avaliações
- Diaskintest. EnglDocumento3 páginasDiaskintest. Englmusicofmylife101Ainda não há avaliações
- Dwi-Tubercular - Uveitis-ThpIIIDocumento24 páginasDwi-Tubercular - Uveitis-ThpIIIAmelinda SdAinda não há avaliações
- Tuberculosis - Natural History, Microbiology, and Pathogenesis - UpToDateDocumento20 páginasTuberculosis - Natural History, Microbiology, and Pathogenesis - UpToDateandreaAinda não há avaliações
- Immunology of MycobacteriumDocumento37 páginasImmunology of MycobacteriumPhablo vinicius dos santos carneiroAinda não há avaliações
- Benito K. Lim Hong III, M.DDocumento55 páginasBenito K. Lim Hong III, M.DCoy NuñezAinda não há avaliações
- Virulence Factor in Tuberculosis: Mycobacterium Tuberculosis Hsp60 As A KeyDocumento16 páginasVirulence Factor in Tuberculosis: Mycobacterium Tuberculosis Hsp60 As A KeyJOSE VAZQUEZ MORALESAinda não há avaliações
- TB PathologyDocumento13 páginasTB PathologyBaqir BroAinda não há avaliações
- Problem Case Tuberculosis)Documento6 páginasProblem Case Tuberculosis)caltzxAinda não há avaliações
- Prepared By:-Kishor R. LalchetaDocumento56 páginasPrepared By:-Kishor R. Lalchetakishor.lalchetaAinda não há avaliações
- Student Project (Unedit)Documento32 páginasStudent Project (Unedit)vikaAinda não há avaliações
- TuberclosisDocumento3 páginasTuberclosisLaith Al ShdifatAinda não há avaliações
- Case Study Template InfluenzaDocumento5 páginasCase Study Template InfluenzaUjjwal MaharjanAinda não há avaliações
- The Role of Gut and Lung Microbiota in SusceptibilityDocumento20 páginasThe Role of Gut and Lung Microbiota in SusceptibilityannewidiatmoAinda não há avaliações
- Mycobacterium TuberculosisDocumento17 páginasMycobacterium TuberculosisKate Anya Buhat-DiesmaAinda não há avaliações
- Wa0006.Documento12 páginasWa0006.Jose VillasmilAinda não há avaliações
- Genoma TBDocumento14 páginasGenoma TBMARIO CASTROAinda não há avaliações
- Micro Chap 21Documento50 páginasMicro Chap 21Farah ZahidAinda não há avaliações
- Hepatic Tuberculosis (New)Documento23 páginasHepatic Tuberculosis (New)khunleangchhun0% (1)
- Mycobacterium TuberculosisDocumento8 páginasMycobacterium TuberculosisDoru RusuAinda não há avaliações
- My Co BacteriumDocumento5 páginasMy Co BacteriumMukiibi MosesAinda não há avaliações
- Host Defense Mechanisms Against Mycobacterium Tuberculosis: Qiyao Chai Zhe Lu Cui Hua LiuDocumento20 páginasHost Defense Mechanisms Against Mycobacterium Tuberculosis: Qiyao Chai Zhe Lu Cui Hua Liurizkarachma64Ainda não há avaliações
- Practical Review of Diagnosis and Management of Cutaneous Tuberculosis in IndonesiaDocumento6 páginasPractical Review of Diagnosis and Management of Cutaneous Tuberculosis in IndonesiaAde Afriza FeraniAinda não há avaliações
- Pathophysiology of Intrathoracic Lymph Node TuberculosisDocumento14 páginasPathophysiology of Intrathoracic Lymph Node TuberculosisNamshaa qureshiAinda não há avaliações
- Description of The MicrobeDocumento3 páginasDescription of The MicrobeMamata GhoshAinda não há avaliações
- 8.TB (Childhood TB)Documento137 páginas8.TB (Childhood TB)auAinda não há avaliações
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocumento18 páginasMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaAinda não há avaliações
- Mycobacterium Tuberculosis: Ecology and Evolution of A Human BacteriumDocumento9 páginasMycobacterium Tuberculosis: Ecology and Evolution of A Human Bacteriumsudipta KhilarAinda não há avaliações
- M.kansasii 2Documento22 páginasM.kansasii 2Ikeh ChisomAinda não há avaliações
- TB PaperDocumento11 páginasTB PapergwapingMDAinda não há avaliações
- Vervloet Et Al-2007-Brazilian Journal of Infectious DiseasesDocumento8 páginasVervloet Et Al-2007-Brazilian Journal of Infectious DiseasesCynthia GalloAinda não há avaliações
- NEJMcibr 0902539Documento3 páginasNEJMcibr 0902539Karen CatariAinda não há avaliações
- 1 s2.0 S1198743X19300813 MainDocumento5 páginas1 s2.0 S1198743X19300813 MainNia KurniawanAinda não há avaliações
- Cytoquine Storm and SepsisDocumento12 páginasCytoquine Storm and SepsisEduardo ChanonaAinda não há avaliações
- S 46 Mladenka TuberculosisDocumento10 páginasS 46 Mladenka TuberculosisCarlo MaxiaAinda não há avaliações
- Mycobacterium: Dr. NG Woei KeanDocumento28 páginasMycobacterium: Dr. NG Woei KeanWong ShuanAinda não há avaliações
- History: Tuberculosis (TB)Documento24 páginasHistory: Tuberculosis (TB)Rashed ShatnawiAinda não há avaliações
- How Does Mycobacterium Tuberculosis EstablishDocumento3 páginasHow Does Mycobacterium Tuberculosis EstablishamiraAinda não há avaliações
- Review Mycobacterium TuberculosisDocumento9 páginasReview Mycobacterium TuberculosisKoyel Sreyashi BasuAinda não há avaliações
- Patogenesis TBDocumento46 páginasPatogenesis TBJaya Semara PutraAinda não há avaliações
- Mycobacterium Tuberculosis: Mycobacterium Tuberculosis Is An Obligate Intracellular Pathogen That IsDocumento5 páginasMycobacterium Tuberculosis: Mycobacterium Tuberculosis Is An Obligate Intracellular Pathogen That IsArdian Zaka RAAinda não há avaliações
- Early Pregnancy Loss - ACOGDocumento23 páginasEarly Pregnancy Loss - ACOGLiviliaMiftaAinda não há avaliações
- Biochimica Et Biophysica Acta: William F. WalkenhorstDocumento10 páginasBiochimica Et Biophysica Acta: William F. WalkenhorstLiviliaMiftaAinda não há avaliações
- Identify Plasmodium Lactate/h+ SymportersDocumento8 páginasIdentify Plasmodium Lactate/h+ SymportersLiviliaMiftaAinda não há avaliações
- Ungulate Malaria ParasitesDocumento8 páginasUngulate Malaria ParasitesLiviliaMiftaAinda não há avaliações
- New Medicine To Improve Medication of MalariaDocumento13 páginasNew Medicine To Improve Medication of MalariaLiviliaMiftaAinda não há avaliações
- Genomic Insight in The Other MalariaDocumento2 páginasGenomic Insight in The Other MalariaLiviliaMiftaAinda não há avaliações
- Fluids and Electrolytes PDFDocumento319 páginasFluids and Electrolytes PDFLiviliaMiftaAinda não há avaliações
- PediDiabeticKetoacidosisManagementProtocol PDFDocumento34 páginasPediDiabeticKetoacidosisManagementProtocol PDFLiviliaMiftaAinda não há avaliações
- Engwerda2013 PDFDocumento3 páginasEngwerda2013 PDFLiviliaMiftaAinda não há avaliações
- Protective Immunity To Liver-Stage Malaria: ReviewDocumento10 páginasProtective Immunity To Liver-Stage Malaria: ReviewLiviliaMiftaAinda não há avaliações
- A Newly Discovered Protein Export Machine in Malaria ParasitesDocumento6 páginasA Newly Discovered Protein Export Machine in Malaria ParasitesLiviliaMiftaAinda não há avaliações
- PediDiabeticKetoacidosisManagementProtocol PDFDocumento34 páginasPediDiabeticKetoacidosisManagementProtocol PDFLiviliaMiftaAinda não há avaliações
- Corticosteeoids in The Treatment of Acute AsthmaDocumento7 páginasCorticosteeoids in The Treatment of Acute AsthmaLiviliaMiftaAinda não há avaliações
- Children With Atopic DermatitisDocumento11 páginasChildren With Atopic DermatitisLiviliaMiftaAinda não há avaliações
- Growth Chart CDC PDFDocumento203 páginasGrowth Chart CDC PDFIrfan FauziAinda não há avaliações
- 00012.pdf Jsessionid PDFDocumento6 páginas00012.pdf Jsessionid PDFLiviliaMiftaAinda não há avaliações
- EBook Episclera and ScleraDocumento18 páginasEBook Episclera and ScleraLiviliaMiftaAinda não há avaliações
- Children With Atopic DermatitisDocumento11 páginasChildren With Atopic DermatitisLiviliaMiftaAinda não há avaliações
- Practice Guidelines For Obstetric Anesthesia PDFDocumento31 páginasPractice Guidelines For Obstetric Anesthesia PDFLiviliaMiftaAinda não há avaliações
- Children With Atopic DermatitisDocumento11 páginasChildren With Atopic DermatitisLiviliaMiftaAinda não há avaliações
- Unit Kajian Dan Maklumat Drug (Ukmd), Husm. Adr Case ReportDocumento56 páginasUnit Kajian Dan Maklumat Drug (Ukmd), Husm. Adr Case ReportRendry Dwitya WirawanAinda não há avaliações
- Cardiac Rehabilitation in Very Old AdultsDocumento6 páginasCardiac Rehabilitation in Very Old AdultsLiviliaMiftaAinda não há avaliações
- Pathophisiology of ItchDocumento8 páginasPathophisiology of ItchLiviliaMiftaAinda não há avaliações
- TB Nejm PDFDocumento25 páginasTB Nejm PDFrisanataliasiburianAinda não há avaliações
- 1 FullDocumento12 páginas1 FullMirona ElenaAinda não há avaliações
- Neurological Examination of Motor SystemDocumento7 páginasNeurological Examination of Motor SystemLiviliaMiftaAinda não há avaliações
- Minnesota State High School LeagueDocumento2 páginasMinnesota State High School Leagueapi-301794844Ainda não há avaliações
- Key Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !Documento6 páginasKey Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !June DumdumayaAinda não há avaliações
- AyurvedicDocumento8 páginasAyurvedicVijay VishwakarmaAinda não há avaliações
- Tutorial Dr. SaugiDocumento33 páginasTutorial Dr. SaugifemmytaniaAinda não há avaliações
- Diseases, Ailments, and Disorders in Urinary System - PPTDocumento24 páginasDiseases, Ailments, and Disorders in Urinary System - PPTIsabella Alycia Lomibao100% (1)
- Problem in Complete Denture Treatment and Postinsertion DentureDocumento35 páginasProblem in Complete Denture Treatment and Postinsertion DentureSorabh JainAinda não há avaliações
- 2017ijmrcr PDFDocumento57 páginas2017ijmrcr PDFIvan InkovAinda não há avaliações
- Organ SpeechDocumento11 páginasOrgan SpeechFaa UlfaaAinda não há avaliações
- Vaccines CHNDocumento2 páginasVaccines CHNLyra LorcaAinda não há avaliações
- D 5 LRDocumento2 páginasD 5 LRDianelie BacenaAinda não há avaliações
- Ophtha LectureDocumento634 páginasOphtha LectureIb YasAinda não há avaliações
- Basic Principles of Animal Form and Function: For Campbell Biology, Ninth EditionDocumento66 páginasBasic Principles of Animal Form and Function: For Campbell Biology, Ninth EditionASEEL AHMADAinda não há avaliações
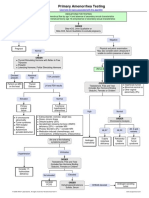
- Primary Amenorrhea Testing AlgorithmDocumento1 páginaPrimary Amenorrhea Testing AlgorithmGabriella AguirreAinda não há avaliações
- Anatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterDocumento75 páginasAnatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterRuth AntolinAinda não há avaliações
- Jaundice Natural RemediesDocumento12 páginasJaundice Natural RemediesprkshshrAinda não há avaliações
- Airway Management 1Documento17 páginasAirway Management 1kamel6Ainda não há avaliações
- Appendectomy Surgery: What Is An Appendix?Documento4 páginasAppendectomy Surgery: What Is An Appendix?Muhammad Ichfan NabiuAinda não há avaliações
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocumento2 páginasPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaAinda não há avaliações
- Housing of Sheep and GoatsDocumento12 páginasHousing of Sheep and Goatsglennpuputi10Ainda não há avaliações
- Snake BitesDocumento21 páginasSnake BitesarifuadAinda não há avaliações
- Are You Kidding MeDocumento10 páginasAre You Kidding MeChelsea RoseAinda não há avaliações
- 9700 m16 Ms 42 PDFDocumento10 páginas9700 m16 Ms 42 PDFsamihaAinda não há avaliações
- Essay-Vegan Vs OmnivorousDocumento3 páginasEssay-Vegan Vs OmnivorousStiven Diaz Florez100% (1)
- Reproduction SystemDocumento38 páginasReproduction SystemNurfatin AdilaAinda não há avaliações
- Variability and Accuracy of Sahlis Method InEstimation of Haemoglobin ConcentrationDocumento8 páginasVariability and Accuracy of Sahlis Method InEstimation of Haemoglobin Concentrationastrii 08Ainda não há avaliações