Você também pode gostar
- Cancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEDocumento25 páginasCancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEece142Ainda não há avaliações
- BAP Guidelines PerinatalDocumento34 páginasBAP Guidelines Perinatalrocsa11Ainda não há avaliações
- Cancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEDocumento9 páginasCancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEece142Ainda não há avaliações
- Alternative Certificate of Foundation Competence - 2018Documento12 páginasAlternative Certificate of Foundation Competence - 2018Chris RaduAinda não há avaliações
- Alternative Certificate of Foundation Competence 2018 Reference GuideDocumento12 páginasAlternative Certificate of Foundation Competence 2018 Reference Guideece142Ainda não há avaliações
- Big Data Approaches To Decomposing Heterogeneity Across The Autism SpectrumDocumento30 páginasBig Data Approaches To Decomposing Heterogeneity Across The Autism Spectrumece142Ainda não há avaliações
- Croft LeafletDocumento2 páginasCroft Leafletece142Ainda não há avaliações
- Alternative Certificate of Foundation Competence 2018 Reference GuideDocumento12 páginasAlternative Certificate of Foundation Competence 2018 Reference Guideece142Ainda não há avaliações
- Mehler2015 Article TreatmentsOfMedicalComplicatioDocumento72 páginasMehler2015 Article TreatmentsOfMedicalComplicatioece142Ainda não há avaliações
- Online Ticket Refund FormDocumento1 páginaOnline Ticket Refund Formece142Ainda não há avaliações
- Evidence of Foundation Competence Applicant Guide 2018Documento6 páginasEvidence of Foundation Competence Applicant Guide 2018ece142Ainda não há avaliações
- 1745 6215 12 175Documento13 páginas1745 6215 12 175ece142Ainda não há avaliações
- Acute Support Allied Health Clinical PrioritisationDocumento4 páginasAcute Support Allied Health Clinical Prioritisationece142Ainda não há avaliações
- Evidence of Foundation Competence Signatory Guide 2018Documento4 páginasEvidence of Foundation Competence Signatory Guide 2018ece142Ainda não há avaliações
- JD Approval ProcessDocumento2 páginasJD Approval Processece142Ainda não há avaliações
- Acute Support Allied Health Clinical PrioritisationDocumento4 páginasAcute Support Allied Health Clinical Prioritisationece142Ainda não há avaliações
- Clinical Characteristics Associated With The Prescribing of SSRI Medication in Adolescents With Major Unipolar..Documento12 páginasClinical Characteristics Associated With The Prescribing of SSRI Medication in Adolescents With Major Unipolar..ece142Ainda não há avaliações
- Mehler2015 Article TreatmentsOfMedicalComplicatio PDFDocumento7 páginasMehler2015 Article TreatmentsOfMedicalComplicatio PDFece142Ainda não há avaliações
- V 031 P 00582Documento5 páginasV 031 P 00582ece142Ainda não há avaliações
- Mehler2015 Article TreatmentsOfMedicalComplicatio PDFDocumento7 páginasMehler2015 Article TreatmentsOfMedicalComplicatio PDFece142Ainda não há avaliações
- WAST 2018 Person Specification June 18Documento3 páginasWAST 2018 Person Specification June 18ece142Ainda não há avaliações
- FP Reference Guide - Key Changes For 2017-1Documento2 páginasFP Reference Guide - Key Changes For 2017-1ece142Ainda não há avaliações
- BAP Guidelines PerinatalDocumento3 páginasBAP Guidelines Perinatalece142Ainda não há avaliações
- Bulimia Nervosa - Medical Complications: Review Open AccessDocumento5 páginasBulimia Nervosa - Medical Complications: Review Open Accessece142Ainda não há avaliações
- Umj7603 177cDocumento1 páginaUmj7603 177cece142Ainda não há avaliações
- Book Reviews: Get Through Mrcophth Part 3: EmqsDocumento2 páginasBook Reviews: Get Through Mrcophth Part 3: Emqsece142Ainda não há avaliações
- BAP Guidelines PerinatalDocumento34 páginasBAP Guidelines Perinatalrocsa11Ainda não há avaliações
- How To Pass MRCPDocumento2 páginasHow To Pass MRCPdooja10100% (2)
- Identification of Disease GenesDocumento24 páginasIdentification of Disease Genesece142Ainda não há avaliações
- Miyagawa Et Al-2015-Human Genome VariationDocumento4 páginasMiyagawa Et Al-2015-Human Genome Variationece142Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- OspndDocumento97 páginasOspndhoangdo11122002Ainda não há avaliações
- MATLAB code for Mann–Kendall test and Sen's slope estimationDocumento7 páginasMATLAB code for Mann–Kendall test and Sen's slope estimationTubaiNandiAinda não há avaliações
- Klasifikasi Industri Perusahaan TercatatDocumento39 páginasKlasifikasi Industri Perusahaan TercatatFz FuadiAinda não há avaliações
- Circulation in Vacuum Pans: January 2004Documento18 páginasCirculation in Vacuum Pans: January 2004REMINGTON SALAYAAinda não há avaliações
- Gil Sanchez, Labason Zamboanga Del Norte: AmacaDocumento2 páginasGil Sanchez, Labason Zamboanga Del Norte: AmacaMacky BirdAinda não há avaliações
- 9643 SoirDocumento38 páginas9643 SoirpolscreamAinda não há avaliações
- Poka Yoke BDocumento31 páginasPoka Yoke BjaymuscatAinda não há avaliações
- NYU Stern Evaluation NewsletterDocumento25 páginasNYU Stern Evaluation NewsletterCanadianValueAinda não há avaliações
- How To Use Oracle Account Generator For Project Related TransactionsDocumento40 páginasHow To Use Oracle Account Generator For Project Related Transactionsapnambiar88Ainda não há avaliações
- GPL 12800 (80) AhDocumento1 páginaGPL 12800 (80) AhismailAinda não há avaliações
- JIG LFO Pack 231 PDFDocumento16 páginasJIG LFO Pack 231 PDFPratiek RaulAinda não há avaliações
- Grate Inlet Skimmer Box ™ (GISB™ ) Suntree Technologies Service ManualDocumento4 páginasGrate Inlet Skimmer Box ™ (GISB™ ) Suntree Technologies Service ManualOmar Rodriguez OrtizAinda não há avaliações
- Wizard's App Pitch Deck by SlidesgoDocumento52 páginasWizard's App Pitch Deck by SlidesgoandreaAinda não há avaliações
- Sequence 2: Greet and Seat The GuestDocumento3 páginasSequence 2: Greet and Seat The GuestNguyễn Ngọc TrâmAinda não há avaliações
- Less Than a Decade to Avoid Catastrophic Climate ChangeDocumento1 páginaLess Than a Decade to Avoid Catastrophic Climate ChangeXie YuJiaAinda não há avaliações
- The Problem and Its SettingDocumento36 páginasThe Problem and Its SettingRodel CamposoAinda não há avaliações
- TT100 Viscometer: For Inline Systems ApplicationsDocumento2 páginasTT100 Viscometer: For Inline Systems ApplicationsPablo Antu Manque RodriguezAinda não há avaliações
- Unit 06 Extra Grammar ExercisesDocumento3 páginasUnit 06 Extra Grammar ExercisesLeo Muñoz43% (7)
- Acuite-India Credit Risk Yearbook FinalDocumento70 páginasAcuite-India Credit Risk Yearbook FinalDinesh RupaniAinda não há avaliações
- Lecture Notes in Airport Engineering PDFDocumento91 páginasLecture Notes in Airport Engineering PDFMaya RajAinda não há avaliações
- Leader in CSR 2020: A Case Study of Infosys LTDDocumento19 páginasLeader in CSR 2020: A Case Study of Infosys LTDDr.Rashmi GuptaAinda não há avaliações
- Loctite 270™: Technical Data SheetDocumento4 páginasLoctite 270™: Technical Data SheetM Jobayer AzadAinda não há avaliações
- 2008 Application FormDocumento12 páginas2008 Application FormVishal PonugotiAinda não há avaliações
- Marantz CD4000 PDFDocumento28 páginasMarantz CD4000 PDFboroda2410Ainda não há avaliações
- Banking Software System Monitoring ToolDocumento4 páginasBanking Software System Monitoring ToolSavun D. CheamAinda não há avaliações
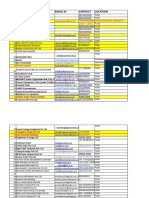
- Company Name Email Id Contact Location: 3 Praj Industries Limited Yogesh960488815Pune-Nagar Road, SanaswadiDocumento65 páginasCompany Name Email Id Contact Location: 3 Praj Industries Limited Yogesh960488815Pune-Nagar Road, SanaswadiDhruv Parekh100% (1)
- How To Block Facebook in Mikrotik Using L7 Protocols (Layer 7) - Lazy Geek - )Documento11 páginasHow To Block Facebook in Mikrotik Using L7 Protocols (Layer 7) - Lazy Geek - )oscar_198810Ainda não há avaliações
- E.R. Hooton, Tom Cooper - Desert Storm - Volume 2 - Operation Desert Storm and The Coalition Liberation of Kuwait 1991 (Middle East@War) (2021, Helion and CompanyDocumento82 páginasE.R. Hooton, Tom Cooper - Desert Storm - Volume 2 - Operation Desert Storm and The Coalition Liberation of Kuwait 1991 (Middle East@War) (2021, Helion and Companydubie dubs100% (5)
- Alcalel-Lucent WLAN OmniAcces StellarDocumento6 páginasAlcalel-Lucent WLAN OmniAcces StellarJBELDAinda não há avaliações
- Philippine Supreme Court Acquits Man of Estafa Due to Lack of KnowledgeDocumento2 páginasPhilippine Supreme Court Acquits Man of Estafa Due to Lack of KnowledgeUrsulaine Grace FelicianoAinda não há avaliações