Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- AbbreviationDocumento19 páginasAbbreviationJayson NatividadAinda não há avaliações
- Doula ContractDocumento2 páginasDoula Contractapi-315824284Ainda não há avaliações
- Updated NDP ReviewerDocumento5 páginasUpdated NDP ReviewerKneth Rye100% (1)
- MS Obstetrics & Gynaecology - Plan of Thesis (Year 2015)Documento4 páginasMS Obstetrics & Gynaecology - Plan of Thesis (Year 2015)RachnaAinda não há avaliações
- Pulmonary Manifestations of Pediatric DiseasesDocumento356 páginasPulmonary Manifestations of Pediatric Diseasesmihaela_bondocAinda não há avaliações
- Nutrition Practice Care Guidelines For Preterm Infants in The CommunityDocumento55 páginasNutrition Practice Care Guidelines For Preterm Infants in The CommunityReine Salamoun100% (1)
- Elderly Primigravida, Adolescent Pregnancy, Grand MultiparaDocumento3 páginasElderly Primigravida, Adolescent Pregnancy, Grand MultiparamercyAinda não há avaliações
- K49 - OG - Caesarean Delivery & Peripartum HysterectomyDocumento45 páginasK49 - OG - Caesarean Delivery & Peripartum HysterectomyMonika AyuningrumAinda não há avaliações
- Cemented Versus UncementedDocumento1 páginaCemented Versus UncementedVAinda não há avaliações
- Aspirin Use and Risk of Hepatocellular Carcinoma in Hepatitis BDocumento2 páginasAspirin Use and Risk of Hepatocellular Carcinoma in Hepatitis BVAinda não há avaliações
- Ca Nasofaring AbstrakDocumento2 páginasCa Nasofaring AbstrakVAinda não há avaliações
- Seminar: William I Wei, Jonathan S T ShamDocumento14 páginasSeminar: William I Wei, Jonathan S T ShamVAinda não há avaliações
- Research in High FlowaDocumento6 páginasResearch in High FlowaVAinda não há avaliações
- Planned Early Birth Versus Expectant Management For WomenDocumento3 páginasPlanned Early Birth Versus Expectant Management For WomenVAinda não há avaliações
- Research in High FlowaDocumento6 páginasResearch in High FlowaVAinda não há avaliações
- Planned Early Birth Versus Expectant Management For WomenDocumento3 páginasPlanned Early Birth Versus Expectant Management For WomenVAinda não há avaliações
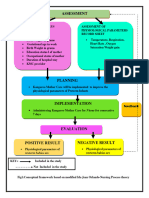
- Defining Characteristic S Nursing Diagnosis Scientific Analysis Plan of Care Nursing Interventions Rationale Subjective: Short Term: IndependentDocumento1 páginaDefining Characteristic S Nursing Diagnosis Scientific Analysis Plan of Care Nursing Interventions Rationale Subjective: Short Term: Independentboomer SeargeAinda não há avaliações
- Per I Natal August 11Documento36 páginasPer I Natal August 11Siti Novita KumanAinda não há avaliações
- DR / Osama Ahmed: Contact UsDocumento20 páginasDR / Osama Ahmed: Contact UsAhmed AliAinda não há avaliações
- CONCEPTUAL FRAN Ida Jean Orlando (3) 46 7Documento5 páginasCONCEPTUAL FRAN Ida Jean Orlando (3) 46 7Roopa KatariaAinda não há avaliações
- Marriott's Employee Engagement Through Preventive HealthDocumento12 páginasMarriott's Employee Engagement Through Preventive HealthShakalya NagAinda não há avaliações
- PCOS Pregnancy RisksDocumento26 páginasPCOS Pregnancy RisksPany Chandra LestariAinda não há avaliações
- RP 00531Documento5 páginasRP 00531Silja ManojAinda não há avaliações
- Chapter 2 For Final PrintingDocumento23 páginasChapter 2 For Final PrintingfreyAinda não há avaliações
- Community WrittenDocumento23 páginasCommunity WrittenImPrint CenterAinda não há avaliações
- Risks of Preterm & Post-Term NewbornsDocumento8 páginasRisks of Preterm & Post-Term NewbornsAngela Del CastilloAinda não há avaliações
- Nicu Case StudyDocumento4 páginasNicu Case Studyapi-508102663Ainda não há avaliações
- Infant of Diabetic MotherDocumento29 páginasInfant of Diabetic MotherChro MAAinda não há avaliações
- Knowledge On Preconception Care Among Reproductive Age WomenDocumento6 páginasKnowledge On Preconception Care Among Reproductive Age WomenMegayanaYessyMarettaAinda não há avaliações
- Pre Test CA3 EPI IMCI Mother and Child With Rationale and Answer 2Documento20 páginasPre Test CA3 EPI IMCI Mother and Child With Rationale and Answer 2Scarlet GrayAinda não há avaliações
- Etiology and Pathogenesis of The Congenital Pneumonia in Newborns Literature Review Part 1 PDFDocumento4 páginasEtiology and Pathogenesis of The Congenital Pneumonia in Newborns Literature Review Part 1 PDFGolden DawnAinda não há avaliações
- Risks of Formula Feeding - A Brief Annotated BibliographyDocumento6 páginasRisks of Formula Feeding - A Brief Annotated BibliographyMireiaAinda não há avaliações
- Practice Guidelines For Music Interventions With Hospitalized Pediatric PatientsDocumento9 páginasPractice Guidelines For Music Interventions With Hospitalized Pediatric PatientsYoon InkiAinda não há avaliações
- Etiology and Outcome of Non-Immune Hydrops Fetalis in Southern China: Report of 1004 CasesDocumento6 páginasEtiology and Outcome of Non-Immune Hydrops Fetalis in Southern China: Report of 1004 CasesMargareta OktavianiAinda não há avaliações
- Clinical Risk Index For Babies (Crib) Ii Score As A Predictor of Neonatal Mortality Among Low Birth Weight Babies at Kenyatta National HospitalDocumento6 páginasClinical Risk Index For Babies (Crib) Ii Score As A Predictor of Neonatal Mortality Among Low Birth Weight Babies at Kenyatta National HospitalVladBadeaAinda não há avaliações
- Breastfeeding Challenges and The Preterm Mother-Infant Dyad A Conceptual ModelDocumento10 páginasBreastfeeding Challenges and The Preterm Mother-Infant Dyad A Conceptual Modelunisa magisterAinda não há avaliações
- Risk factors for childhood epilepsy in SyriaDocumento8 páginasRisk factors for childhood epilepsy in Syrianurhasanah nanaAinda não há avaliações
- PREMATURITYDocumento40 páginasPREMATURITYBlykeBantuganAinda não há avaliações