Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- EMS Systems in KoreaDocumento4 páginasEMS Systems in KoreaJamison ParfittAinda não há avaliações
- INFANT FBAO Management Skills Evaluation - 2022Documento1 páginaINFANT FBAO Management Skills Evaluation - 2022Ryan Joseph ConcepcionAinda não há avaliações
- ASHI ACLS Form Field FlyerDocumento1 páginaASHI ACLS Form Field FlyerErwin RomeroAinda não há avaliações
- TEAM MEDIC DRILLS v4Documento11 páginasTEAM MEDIC DRILLS v4Jimmy JamesAinda não há avaliações
- CPR For DogsDocumento2 páginasCPR For DogstravtedAinda não há avaliações
- List of Empanelled HCOs-Pune (Dec 2020)Documento15 páginasList of Empanelled HCOs-Pune (Dec 2020)GATE FACULTYAinda não há avaliações
- Basic Life Support: Cardiopulmonary Resuscitation Prepared By: BSN - 3Documento20 páginasBasic Life Support: Cardiopulmonary Resuscitation Prepared By: BSN - 3sheryline100% (1)
- Triage in Mass Casualty IncidentsDocumento55 páginasTriage in Mass Casualty Incidentsluis_chubeeAinda não há avaliações
- DefibrilatorDocumento24 páginasDefibrilatorMoonGalaxyAinda não há avaliações
- National Law University Odisha, Cuttack: Topic: Apollo PharmacyDocumento55 páginasNational Law University Odisha, Cuttack: Topic: Apollo PharmacyAbhijeet SahooAinda não há avaliações
- Sotry Board Dan ScriptDocumento4 páginasSotry Board Dan Scriptnuex01Ainda não há avaliações
- E PneumothoraxDocumento12 páginasE PneumothoraxErna MiraniAinda não há avaliações
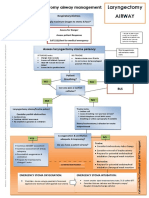
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocumento1 páginaLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieAinda não há avaliações
- Open FractureDocumento9 páginasOpen FractureAnnyl LaurelAinda não há avaliações
- AJCMWinter 20092Documento52 páginasAJCMWinter 20092William L McGillAinda não há avaliações
- Materi Senja Setiaka S.kep. Ns.Documento184 páginasMateri Senja Setiaka S.kep. Ns.BernardAinda não há avaliações
- Lsti Emt B ManualDocumento190 páginasLsti Emt B ManualPonzidiane123Ainda não há avaliações
- A ListaDocumento31 páginasA Listaking_petarAinda não há avaliações
- U L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry OurseDocumento9 páginasU L S E C - Usls Bl1-P: Ltrasound IFE Upport Ntry Oursesaraswaty710Ainda não há avaliações
- RLS Hemorrhage ControlDocumento38 páginasRLS Hemorrhage ControlMela IsnaeniAinda não há avaliações
- Set Rec Pic 829Documento2 páginasSet Rec Pic 829Peter SalimAinda não há avaliações
- HemorrhageDocumento15 páginasHemorrhageMariegreat Piscos BisnarAinda não há avaliações
- CPR LectureDocumento10 páginasCPR LecturejacnpoyAinda não há avaliações
- Triage Question BankDocumento5 páginasTriage Question BankKusuma Edhi Kuncoro0% (1)
- The Importance of TourniquetsDocumento124 páginasThe Importance of Tourniquetsjlipa100% (1)
- Techniques of Helmet Removal From Injured Patients: April 1997Documento4 páginasTechniques of Helmet Removal From Injured Patients: April 1997Ricardo Luis Martin Sant'AnnaAinda não há avaliações
- Interview Questions For NursesDocumento2 páginasInterview Questions For Nursesshalf0xAinda não há avaliações
- Letter To CouncilDocumento10 páginasLetter To CouncilCHAT NEWSAinda não há avaliações
- Skills You Need To Learn First Aid Survival Skills Checklist 1 1Documento3 páginasSkills You Need To Learn First Aid Survival Skills Checklist 1 1Agustin PeraltaAinda não há avaliações
- CPR ChecklistDocumento2 páginasCPR ChecklistJenny Agustin Fabros100% (2)