Você também pode gostar
- Mallampati Airway ClassificationDocumento6 páginasMallampati Airway ClassificationAnthony Osemudiamen OseghaleAinda não há avaliações
- Open I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityDocumento21 páginasOpen I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityPOTENCIANA MAROMAAinda não há avaliações
- Osce Stations - Blogspot.com Paediatric Respiratory ExamDocumento2 páginasOsce Stations - Blogspot.com Paediatric Respiratory ExamrohitAinda não há avaliações
- Osce Stations - Blogspot.com Paediatric Respiratory ExamDocumento2 páginasOsce Stations - Blogspot.com Paediatric Respiratory ExamrohitAinda não há avaliações
- ATLFFDocumento2 páginasATLFFPrameswari ZahidaAinda não há avaliações
- Peds IDCBR ReviewDocumento1 páginaPeds IDCBR ReviewshreeAinda não há avaliações
- Neonatal Examination: 2016 EditionDocumento18 páginasNeonatal Examination: 2016 EditionDoha100% (1)
- Pancreatitis PathwayDocumento31 páginasPancreatitis PathwaybernadeteAinda não há avaliações
- Physical Assessment (Head and Mouth)Documento3 páginasPhysical Assessment (Head and Mouth)Marie Nelle Escriba Limpoco100% (1)
- FACE ExercisesDocumento9 páginasFACE Exercisesmandeep axonAinda não há avaliações
- Ds Sinonasal PolyposisDocumento3 páginasDs Sinonasal PolyposisJayahar AlexanderAinda não há avaliações
- CASE Study ENCEPHALITISDocumento29 páginasCASE Study ENCEPHALITISMeena Koushal67% (3)
- Swallowing ChecklistsDocumento5 páginasSwallowing ChecklistsTaylor MayAinda não há avaliações
- Obstetric Physical ExaminationDocumento2 páginasObstetric Physical ExaminationNor Atikah EnddyAinda não há avaliações
- Ds Left CsomDocumento4 páginasDs Left CsomJayahar AlexanderAinda não há avaliações
- Pedia - Case Analysis - Dengue. Sakin 2docxDocumento22 páginasPedia - Case Analysis - Dengue. Sakin 2docxMhackie PerezAinda não há avaliações
- Down Syndrome: Songkran Andaya, Santos & MendozaDocumento16 páginasDown Syndrome: Songkran Andaya, Santos & MendozaHyacinthjade SantosAinda não há avaliações
- Newborn Assessment Turn inDocumento7 páginasNewborn Assessment Turn inapi-234767222Ainda não há avaliações
- Congenital Anomalies in Newborn (Critical)Documento46 páginasCongenital Anomalies in Newborn (Critical)Shereen Mohamed Soliman HammoudaAinda não há avaliações
- Advanced Assessments Final ExamDocumento57 páginasAdvanced Assessments Final ExamBreanna BeckfordAinda não há avaliações
- Nursing Care Plan-EpilepsyDocumento24 páginasNursing Care Plan-Epilepsyamit82% (11)
- Newborn AssessmentDocumento9 páginasNewborn Assessmentapi-237668254Ainda não há avaliações
- NR 304 - Health Assessment II Head To Toe Assessment Final Script Introduction & AIDETDocumento14 páginasNR 304 - Health Assessment II Head To Toe Assessment Final Script Introduction & AIDETA Sung100% (5)
- Ds TonsillectomyDocumento3 páginasDs TonsillectomyJayahar AlexanderAinda não há avaliações
- BG TQ RHM - Chỉnh nhaDocumento42 páginasBG TQ RHM - Chỉnh nhaThanh MaiiAinda não há avaliações
- Final Year Clinicals: Malocclusions and Etiology (Graber)Documento31 páginasFinal Year Clinicals: Malocclusions and Etiology (Graber)Sruthy NairAinda não há avaliações
- Deviated Nasal Septum: Nandini V 3 Year Bgs GimsDocumento22 páginasDeviated Nasal Septum: Nandini V 3 Year Bgs Gimsr7ptzc5kcmAinda não há avaliações
- 2015 - Hypospadias SurgeryDocumento16 páginas2015 - Hypospadias SurgerytiaraAinda não há avaliações
- Case 9 - MucoceleDocumento56 páginasCase 9 - MucoceleSAGAR ADHIKARIAinda não há avaliações
- PediaDocumento13 páginasPediareooooAinda não há avaliações
- Occlusal Anomalies Abnormal Occlusion MalocclusionDocumento8 páginasOcclusal Anomalies Abnormal Occlusion Malocclusionapi-19840404Ainda não há avaliações
- SnorlaaaxDocumento15 páginasSnorlaaaxPinklet Arleena CubianAinda não há avaliações
- Case Presentation DraftDocumento6 páginasCase Presentation DraftGwendareign ElizanAinda não há avaliações
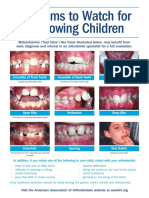
- Problems To Watch For in Growing ChildrenDocumento2 páginasProblems To Watch For in Growing ChildrenMonica S. Alcouce TannerAinda não há avaliações
- Case PresentationDocumento16 páginasCase PresentationJIESEL ACEBEDOAinda não há avaliações
- Cerebral Aneurysm FINALDocumento33 páginasCerebral Aneurysm FINALkanejasper0% (2)
- PAT Score UpdateDocumento2 páginasPAT Score UpdateTATIAinda não há avaliações
- Please Note: This Information Is About Kids. Not Adult Abnormal Swallowing HabitsDocumento4 páginasPlease Note: This Information Is About Kids. Not Adult Abnormal Swallowing HabitsLore DanAinda não há avaliações
- English Papers (Cva)Documento18 páginasEnglish Papers (Cva)yusminaAinda não há avaliações
- Bronchopneumonia: Prepared By: Bsn-3B-0Documento64 páginasBronchopneumonia: Prepared By: Bsn-3B-0Mark Norriel CajandabAinda não há avaliações
- Ceasarean Case StudyDocumento26 páginasCeasarean Case StudyNarissa Jay Taub YlananAinda não há avaliações
- HabitsDocumento67 páginasHabitsMehak AryaAinda não há avaliações
- Eyes - Ears - Mouth - Nose (Lecture 5)Documento50 páginasEyes - Ears - Mouth - Nose (Lecture 5)اسامة محمد السيد رمضانAinda não há avaliações
- Budi - Cleft Lip and PalateDocumento70 páginasBudi - Cleft Lip and PalateShalsa NabillaAinda não há avaliações
- Head Neck and Skin Assessment Cheat SheetDocumento3 páginasHead Neck and Skin Assessment Cheat SheetcarlyAinda não há avaliações
- Diagnosis & Treatment Planning of Completely Edentulous PatientsDocumento61 páginasDiagnosis & Treatment Planning of Completely Edentulous Patientsa,sajsdoqjsAinda não há avaliações
- Neonatal Assessment FormDocumento3 páginasNeonatal Assessment FormLeen ShweikiAinda não há avaliações
- Orthodontic AssessmentDocumento59 páginasOrthodontic AssessmentSyaifuddin ADamAinda não há avaliações
- Open BiteDocumento32 páginasOpen BiteMohammed Al-MusawiAinda não há avaliações
- Examination Medicine: General Systems ChapterDocumento17 páginasExamination Medicine: General Systems ChapterMahmoud AbouelsoudAinda não há avaliações
- Mrs. Carolyn L. Bote: Clinical InstructorDocumento36 páginasMrs. Carolyn L. Bote: Clinical InstructorbearosAinda não há avaliações
- Nursery Assessment FormDocumento4 páginasNursery Assessment FormRuben, Jun Carlo C.Ainda não há avaliações
- Abdo History TakingDocumento4 páginasAbdo History TakingJamie Rina KeeAinda não há avaliações
- Heent: Section F Group 1 Subgroup 3Documento67 páginasHeent: Section F Group 1 Subgroup 3Mhanlhyn QuiñonesAinda não há avaliações
- Non Verbal CommunicationDocumento72 páginasNon Verbal CommunicationNikita NikitaAinda não há avaliações
- General Survey and Integumentary I. General Appearance and Mental Status Normal Findings Actual Findings Analysis and InterpretationDocumento9 páginasGeneral Survey and Integumentary I. General Appearance and Mental Status Normal Findings Actual Findings Analysis and InterpretationAllana RayosAinda não há avaliações
- Case Study: Periorbital Cellulitis To Consider AbcessDocumento11 páginasCase Study: Periorbital Cellulitis To Consider AbcessPriscilla ChantalAinda não há avaliações
- Case Study On Meninomyocele (Repaired) PDocumento29 páginasCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Premature BabyDocumento41 páginasPremature BabyVijith.V.kumar100% (9)
- 婦兒combine 15480514 陳o柔之子B Cleft Lip and Palate, Suspect Sturge-Weber Syndrome or Klippel-Trenaunay Syndrome-劉庭維Documento29 páginas婦兒combine 15480514 陳o柔之子B Cleft Lip and Palate, Suspect Sturge-Weber Syndrome or Klippel-Trenaunay Syndrome-劉庭維鄧沛元醫師Ainda não há avaliações
- EfektivitasDocumento35 páginasEfektivitasyulianakiranaAinda não há avaliações
- Health 2Documento7 páginasHealth 2yulianakiranaAinda não há avaliações
- DentlDocumento3 páginasDentlyulianakiranaAinda não há avaliações
- EfektivitasDocumento35 páginasEfektivitasyulianakiranaAinda não há avaliações
- Pharmacon Open Journal Systems Journal Help User Username Password Remember Me NotificationsDocumento4 páginasPharmacon Open Journal Systems Journal Help User Username Password Remember Me NotificationsyulianakiranaAinda não há avaliações
- Dental Hygienist: Job DescriptionDocumento5 páginasDental Hygienist: Job DescriptionyulianakiranaAinda não há avaliações
- EfektivitasDocumento35 páginasEfektivitasyulianakiranaAinda não há avaliações
- EfektivitasDocumento35 páginasEfektivitasyulianakiranaAinda não há avaliações
- EfektivitasDocumento35 páginasEfektivitasyulianakiranaAinda não há avaliações
- EfektivitasDocumento35 páginasEfektivitasyulianakiranaAinda não há avaliações
- Pharmacon Open Journal Systems Journal Help User Username Password Remember Me NotificationsDocumento4 páginasPharmacon Open Journal Systems Journal Help User Username Password Remember Me NotificationsyulianakiranaAinda não há avaliações
- MyobraceDocumento2 páginasMyobraceyulianakiranaAinda não há avaliações
- Pharmacon Open Journal Systems Journal Help User Username Password Remember Me NotificationsDocumento4 páginasPharmacon Open Journal Systems Journal Help User Username Password Remember Me NotificationsyulianakiranaAinda não há avaliações
- Good Practitioners Guide 2016 PDFDocumento52 páginasGood Practitioners Guide 2016 PDFKarolis K100% (1)
- Form Jawaban Kuesioner PenjarkesDocumento1 páginaForm Jawaban Kuesioner PenjarkesyulianakiranaAinda não há avaliações
- ScribdDocumento16 páginasScribdyulianakiranaAinda não há avaliações
- MyobraceDocumento2 páginasMyobraceyulianakiranaAinda não há avaliações
- Dental Hygienist Chronicles Her Journey Into Orofacial Myofunctional TherapyDocumento12 páginasDental Hygienist Chronicles Her Journey Into Orofacial Myofunctional TherapyyulianakiranaAinda não há avaliações
- Algeria Country PaperDocumento9 páginasAlgeria Country PaperSandeep MahantaAinda não há avaliações
- Importance of Strengthening Your Core MusclesDocumento6 páginasImportance of Strengthening Your Core Musclesallan_apduaAinda não há avaliações
- Cardio VascularDocumento42 páginasCardio VascularMamta ShuklaAinda não há avaliações
- Comparative Evaluation Between F1 Duroc HampshireDocumento9 páginasComparative Evaluation Between F1 Duroc HampshireGed L'EsparverAinda não há avaliações
- Hematology 1 MidtermsDocumento31 páginasHematology 1 Midtermsella SyAinda não há avaliações
- Ancient India-1: Pre-History: Complementary Initiative Under Current Affairs ProgramDocumento9 páginasAncient India-1: Pre-History: Complementary Initiative Under Current Affairs ProgramRaj kumarAinda não há avaliações
- Biology Paper 2 16 Tests M SDocumento64 páginasBiology Paper 2 16 Tests M SMakembu Wa MwangiAinda não há avaliações
- Review of Indigenous Sheep Breeds Production Systems in EthiopiaDocumento7 páginasReview of Indigenous Sheep Breeds Production Systems in EthiopiaInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- OrionpptDocumento20 páginasOrionpptJoggie Mae MagarzoAinda não há avaliações
- CASE PRE (Intrapartum)Documento6 páginasCASE PRE (Intrapartum)teuuuuAinda não há avaliações
- The Five Human SensesDocumento17 páginasThe Five Human SensesAntonio Gonzalez100% (1)
- Keep Up With Feeding And/or Pasture Management. You Cannot Raise Cattle If You Have Nothing To Feed Them orDocumento8 páginasKeep Up With Feeding And/or Pasture Management. You Cannot Raise Cattle If You Have Nothing To Feed Them orMarie Lyca Dela CruzAinda não há avaliações
- Three Faces of Hecate - Ritual PDFDocumento3 páginasThree Faces of Hecate - Ritual PDFEric TuckerAinda não há avaliações
- Product Catalogue 2010Documento112 páginasProduct Catalogue 2010Dennis NguyenAinda não há avaliações
- Step 2 CasesDocumento0 páginaStep 2 CasesSergio VillaAinda não há avaliações
- TASK SHEET No. 1.2-1 Title: Perform Different Knots Used in Restraining Animals Performance ObjectiveDocumento7 páginasTASK SHEET No. 1.2-1 Title: Perform Different Knots Used in Restraining Animals Performance ObjectiveRoh NaldzAinda não há avaliações
- Deteksi Seksual Dimorfisme Pada Benih Ikan Tawes (Barbomymus Gonionotus Bleeker, 1850) Berdasarkan Morfologi Dan AnatomiDocumento13 páginasDeteksi Seksual Dimorfisme Pada Benih Ikan Tawes (Barbomymus Gonionotus Bleeker, 1850) Berdasarkan Morfologi Dan AnatomiSiwiana Dinar UtaminingtyasAinda não há avaliações
- Capitolul 7Documento6 páginasCapitolul 7Monica EnescuAinda não há avaliações
- OSCE - Chest PainDocumento2 páginasOSCE - Chest PaincgalongAinda não há avaliações
- FOM STUDY GUIDE 3rd Block 1Documento3 páginasFOM STUDY GUIDE 3rd Block 1Bernadine Cruz Par100% (1)
- Reinforcement and Extension 2Documento12 páginasReinforcement and Extension 2Patri Pardellas BlunierAinda não há avaliações
- To Be/ Have Got Test (A1)Documento2 páginasTo Be/ Have Got Test (A1)Velislava IvanovaAinda não há avaliações
- 6.2 RT Summarizing PracticeDocumento5 páginas6.2 RT Summarizing PracticeMoulay Mohamed (Student) Bouabd ElliAinda não há avaliações
- Popcorn Lamb Amigurumi Crochet PDF Free PatternDocumento7 páginasPopcorn Lamb Amigurumi Crochet PDF Free Patternami arinta100% (1)
- Basic Anatomy and Physiology of Brain and Spinal CordDocumento59 páginasBasic Anatomy and Physiology of Brain and Spinal CorddrmalikarifAinda não há avaliações
- Generic Dungeon WOTCDocumento9 páginasGeneric Dungeon WOTCMark YfjAinda não há avaliações
- National Geographic - May (2010) (Malestrom)Documento81 páginasNational Geographic - May (2010) (Malestrom)GAinda não há avaliações
- African Grey Parrot - WikipediaDocumento3 páginasAfrican Grey Parrot - WikipediaWilhelm Richard WagnerAinda não há avaliações
- Unisystem PiratesDocumento8 páginasUnisystem PiratesAnime300100% (1)
- Zak's Class SystemDocumento115 páginasZak's Class SystemGeorge Quail100% (2)