Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Comprehensive Guide to Migraine: Causes, Symptoms and TreatmentDocumento29 páginasComprehensive Guide to Migraine: Causes, Symptoms and TreatmentNatalie MbonjaniAinda não há avaliações
- 0199605602Documento318 páginas0199605602Eudon MuliawanAinda não há avaliações
- Neurology Clerkship Study GuideDocumento84 páginasNeurology Clerkship Study GuideHilary Steele100% (1)
- Yyyyy Y YDocumento49 páginasYyyyy Y YSiva Nantham100% (1)
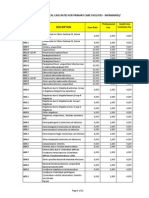
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocumento22 páginasPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraAinda não há avaliações
- Ménière's Disease: Vertigo - Hearing Loss - Tinnitus: A Psychosomatically Oriented Presentation Helmut SchaafDocumento304 páginasMénière's Disease: Vertigo - Hearing Loss - Tinnitus: A Psychosomatically Oriented Presentation Helmut SchaafG PalaAinda não há avaliações
- Final Written ENT With CoverDocumento231 páginasFinal Written ENT With CoverAlyAl-MakhzangyAinda não há avaliações
- Ent MCQ 20000 PDFDocumento19 páginasEnt MCQ 20000 PDFIvana Supit60% (5)
- GI AND ENO QUESTIONERDocumento26 páginasGI AND ENO QUESTIONERRymmus Asuncion100% (1)
- Managing ENT DisordersDocumento26 páginasManaging ENT DisordersShreyas Walvekar100% (3)
- Edoskopi FleksibelDocumento4 páginasEdoskopi FleksibelDex RayAinda não há avaliações
- Disfagia Pasca RadioterapiDocumento8 páginasDisfagia Pasca RadioterapiDex RayAinda não há avaliações
- Brain Abscess Management: Presenter: Pankaj Ailawadhi Moderators: PROF. BS SHARMA Dr. Sumit SinhaDocumento86 páginasBrain Abscess Management: Presenter: Pankaj Ailawadhi Moderators: PROF. BS SHARMA Dr. Sumit SinhaDex RayAinda não há avaliações
- Sensory Examination DefinitionsDocumento13 páginasSensory Examination DefinitionsDex RayAinda não há avaliações
- Guideline Prevention Venous ThromboembolismDocumento157 páginasGuideline Prevention Venous ThromboembolismDex RayAinda não há avaliações
- The Management of DVT - The Autar PDFDocumento11 páginasThe Management of DVT - The Autar PDFFayza Rihastara100% (1)
- Deep-Vein Thrombosis PDFDocumento25 páginasDeep-Vein Thrombosis PDFDex RayAinda não há avaliações
- Deep Vein ThrombisisDocumento13 páginasDeep Vein ThrombisisDex RayAinda não há avaliações
- Dengue Guideline DengueDocumento33 páginasDengue Guideline DenguedrkkdbAinda não há avaliações
- Gagal GinjalDocumento34 páginasGagal GinjalDex RayAinda não há avaliações
- Guidelines On Clinical Management DFDHF2009Documento44 páginasGuidelines On Clinical Management DFDHF2009Desti PasmawatiAinda não há avaliações
- Denguide LabDocumento10 páginasDenguide LabHeide Danica A. BaltazarAinda não há avaliações
- Vocab U LarryDocumento3 páginasVocab U LarryDex RayAinda não há avaliações
- Subjective Visual Vertical in Vestibular Disorders Measured With The Bucket TestDocumento9 páginasSubjective Visual Vertical in Vestibular Disorders Measured With The Bucket Testcamila hernandezAinda não há avaliações
- Advances in Vestibular Rehabilitation: Shaleen Sulway Susan L. WhitneyDocumento6 páginasAdvances in Vestibular Rehabilitation: Shaleen Sulway Susan L. WhitneymykedindealAinda não há avaliações
- Approach To AtaxiaDocumento6 páginasApproach To AtaxiaVivek KumarAinda não há avaliações
- Vertigo and ImbalanceDocumento19 páginasVertigo and ImbalanceDiena HarisahAinda não há avaliações
- Motion Sickness Its Pathophysiology and TreatmentDocumento7 páginasMotion Sickness Its Pathophysiology and TreatmentimmanueldioAinda não há avaliações
- Main ICM Shelf Exam (2012 Nov MUA)Documento8 páginasMain ICM Shelf Exam (2012 Nov MUA)mentawistAinda não há avaliações
- DizzinessDocumento6 páginasDizzinessRebecca WongAinda não há avaliações
- Benign Paroxysmal Positional Vertigo (BPPV)Documento91 páginasBenign Paroxysmal Positional Vertigo (BPPV)UjjawalShriwastavAinda não há avaliações
- NeuroMisc NotesDocumento17 páginasNeuroMisc Notessmian08Ainda não há avaliações
- Dizziness and Balance ProblemsDocumento20 páginasDizziness and Balance ProblemsSeldon GoAinda não há avaliações
- NeurologiaDocumento216 páginasNeurologiaPietro BracagliaAinda não há avaliações
- Vertigo BPPV Benign VertigoDocumento6 páginasVertigo BPPV Benign Vertigoaokan@hotmail.comAinda não há avaliações
- Central VertigoDocumento9 páginasCentral VertigoDiayanti TentiAinda não há avaliações
- Overview of The Anatomy and Physiology: AuditionDocumento16 páginasOverview of The Anatomy and Physiology: AuditionEm Hernandez AranaAinda não há avaliações
- Una CoalesDocumento394 páginasUna Coalesabuzeid5100% (1)
- ENT CourseDocumento29 páginasENT Coursetaliya. shvetzAinda não há avaliações
- #Complications of Suppurative Otitis MediaDocumento8 páginas#Complications of Suppurative Otitis MediaameerabestAinda não há avaliações
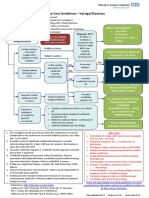
- ENT Vertigo FINAL v0.41Documento1 páginaENT Vertigo FINAL v0.41Farmasi BhamadaAinda não há avaliações
- Dr. Chitale ENT Hospital - Vertigo Center in PuneDocumento5 páginasDr. Chitale ENT Hospital - Vertigo Center in PuneDr. Vinaya ChitaleAinda não há avaliações
- Scott III OtologyDocumento604 páginasScott III OtologyDr-Firas Nayf Al-ThawabiaAinda não há avaliações