Você também pode gostar
- The China Study: The Most Comprehensive Study of Nutrition Ever Conducted and the Startling Implications for Diet, Weight Loss and Long-term Health by T. Colin Campbell and Thomas M. Campbell, II | Key Takeaways, Analysis & ReviewNo EverandThe China Study: The Most Comprehensive Study of Nutrition Ever Conducted and the Startling Implications for Diet, Weight Loss and Long-term Health by T. Colin Campbell and Thomas M. Campbell, II | Key Takeaways, Analysis & ReviewNota: 5 de 5 estrelas5/5 (1)
- Early Aggressive Nutrition Improves Growth in Premature InfantsDocumento5 páginasEarly Aggressive Nutrition Improves Growth in Premature InfantsFlaming NbAinda não há avaliações
- Am J Clin Nutr 2007 Fewtrell 635S 8SggDocumento4 páginasAm J Clin Nutr 2007 Fewtrell 635S 8SggMariaAinda não há avaliações
- 546f2ba60cf216f8cfa94f21 PDFDocumento11 páginas546f2ba60cf216f8cfa94f21 PDFjohanesAinda não há avaliações
- Nutrients 09 00520Documento9 páginasNutrients 09 00520husynAinda não há avaliações
- Improving Nutrition Outcomes For Infants With A Progressive, Evidenced-Based Enteral Feeding ProtocolDocumento9 páginasImproving Nutrition Outcomes For Infants With A Progressive, Evidenced-Based Enteral Feeding ProtocolgianellaAinda não há avaliações
- Infant Feeding and Feeding Transitions During The First Year of LifeDocumento9 páginasInfant Feeding and Feeding Transitions During The First Year of LifeVinitha DsouzaAinda não há avaliações
- BLW 2018 DoganDocumento25 páginasBLW 2018 DoganGenesis VelizAinda não há avaliações
- Developmental Status of 1-Year-Old Infants Fed Breast Milk, Cow 'S Milk Formula, or Soy FormulaDocumento7 páginasDevelopmental Status of 1-Year-Old Infants Fed Breast Milk, Cow 'S Milk Formula, or Soy FormulaDesty Adjaahh LaahhAinda não há avaliações
- Clinical Research: Outcomes of Early Nutrition Support in Extremely Low-Birth-Weight InfantsDocumento6 páginasClinical Research: Outcomes of Early Nutrition Support in Extremely Low-Birth-Weight InfantsgianellaAinda não há avaliações
- Artikel EBF & CFDocumento7 páginasArtikel EBF & CFdayana nopridaAinda não há avaliações
- Pediatric JournalDocumento9 páginasPediatric JournalSatrianiAinda não há avaliações
- Maternal obesity and high-fat diet program offspring metabolic syndromeDocumento13 páginasMaternal obesity and high-fat diet program offspring metabolic syndromeMuhammad BasriAinda não há avaliações
- Type of Infant Formula in Weight and Length DifferencesDocumento11 páginasType of Infant Formula in Weight and Length DifferencesJade IreneAinda não há avaliações
- Pediatrics 2012 Andres 1134 40Documento9 páginasPediatrics 2012 Andres 1134 40Anggie DeayuAinda não há avaliações
- Northwest Mothers Milk BankDocumento12 páginasNorthwest Mothers Milk Bankapi-241882918Ainda não há avaliações
- Am J Clin Nutr 2007 Fewtrell 635S 8SDocumento4 páginasAm J Clin Nutr 2007 Fewtrell 635S 8SpiterwiselyAinda não há avaliações
- Effect of Early Parenteral Nutrition Discontinuation on Time to Regain Birth WeightDocumento8 páginasEffect of Early Parenteral Nutrition Discontinuation on Time to Regain Birth WeightmerindaAinda não há avaliações
- E20160772 FullDocumento10 páginasE20160772 FullRaehana AlaydrusAinda não há avaliações
- BLWDocumento12 páginasBLWNicole Andrea Peña RodríguezAinda não há avaliações
- Association Between Rooming-In Policy and Neonatal HyperbilirubinemiaDocumento6 páginasAssociation Between Rooming-In Policy and Neonatal HyperbilirubinemiaRissa IchaAinda não há avaliações
- 13 Ashwinee EtalDocumento5 páginas13 Ashwinee EtaleditorijmrhsAinda não há avaliações
- Association PDFDocumento4 páginasAssociation PDFLia RusmanAinda não há avaliações
- Prolonged Breast-Feeding: No Association With Increased Risk of Clinical Malnutrition in Young Children in Burkina FasoDocumento10 páginasProlonged Breast-Feeding: No Association With Increased Risk of Clinical Malnutrition in Young Children in Burkina FasoranihajriAinda não há avaliações
- 18381-Article Text-59445-1-10-20171011Documento6 páginas18381-Article Text-59445-1-10-20171011maxmaxAinda não há avaliações
- Oral sensorimotor intervention enhances breastfeeding in preemiesDocumento8 páginasOral sensorimotor intervention enhances breastfeeding in preemiesAries CamiAinda não há avaliações
- 1 s2.0 S0022347616004376 MainDocumento7 páginas1 s2.0 S0022347616004376 MainRatih KusumawardaniAinda não há avaliações
- Improved Nutrition Delivery and Nutrition Status in Critically Ill Children With Heart DiseaseDocumento9 páginasImproved Nutrition Delivery and Nutrition Status in Critically Ill Children With Heart DiseasedaindesAinda não há avaliações
- Amino Acid LBWBDocumento6 páginasAmino Acid LBWBWiwit ClimberAinda não há avaliações
- J Pediatr Gastroenterol NutrDocumento1 páginaJ Pediatr Gastroenterol NutrHellen AbreuAinda não há avaliações
- Benefits of Early Enteral Nutrition in Extremely LowDocumento18 páginasBenefits of Early Enteral Nutrition in Extremely LowTya VenyAinda não há avaliações
- Influence of Breast-Feeding On Weight Loss, Jaundice, and Waste Elimination in NeonatesDocumento8 páginasInfluence of Breast-Feeding On Weight Loss, Jaundice, and Waste Elimination in NeonatesCristina SánchezAinda não há avaliações
- Nresearch PaperDocumento14 páginasNresearch Paperapi-400982160Ainda não há avaliações
- Achievement of full enteral feeding in preterm infants using volume advancementDocumento5 páginasAchievement of full enteral feeding in preterm infants using volume advancementrexaAinda não há avaliações
- Paediatrica Indonesiana: Teti Hendrayani, Afifa Ramadanti, Indrayady, Raden Muhammad IndraDocumento5 páginasPaediatrica Indonesiana: Teti Hendrayani, Afifa Ramadanti, Indrayady, Raden Muhammad IndrarexaAinda não há avaliações
- Pack Alimentacion Clin in Perin 14Documento194 páginasPack Alimentacion Clin in Perin 14Paz BustosAinda não há avaliações
- Early Feeding: Lifelong Health: Questions and Answers From BNF WebinarDocumento3 páginasEarly Feeding: Lifelong Health: Questions and Answers From BNF WebinarMantas LiekisAinda não há avaliações
- Frequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeDocumento3 páginasFrequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeAndhika SatriyaAinda não há avaliações
- Bifidobacterium and Enteral Feeding in Preterm Infants: Cluster-Randomized TrialDocumento6 páginasBifidobacterium and Enteral Feeding in Preterm Infants: Cluster-Randomized TrialnashwaAinda não há avaliações
- Prebiotic Supplementation Improves Apetite Control in Children With Overweight and Obesity, A Randomized Controlled TrialDocumento11 páginasPrebiotic Supplementation Improves Apetite Control in Children With Overweight and Obesity, A Randomized Controlled TrialJUAN SEBASTIAN AVELLANEDA MARTINEZAinda não há avaliações
- Journal of Nutritional ScienceDocumento11 páginasJournal of Nutritional ScienceDipo YudistiraAinda não há avaliações
- JNB 1 306Documento8 páginasJNB 1 306akshayajainaAinda não há avaliações
- Is Breastfeeding Really Favoring Early Neonatal Jaundice?: Pediatrics April 2001Documento8 páginasIs Breastfeeding Really Favoring Early Neonatal Jaundice?: Pediatrics April 2001Jeklee MancapAinda não há avaliações
- Excessive Weight Gain Followed by Catch-Down in Ex PDFDocumento20 páginasExcessive Weight Gain Followed by Catch-Down in Ex PDFPATRICIA QUAGLIAAinda não há avaliações
- Nresearch PaperDocumento13 páginasNresearch Paperapi-399638162Ainda não há avaliações
- 1 s2.0 S0021755721000991 MainDocumento8 páginas1 s2.0 S0021755721000991 MainF Gonzales XtlvAinda não há avaliações
- Pi Is 0022347613009517Documento3 páginasPi Is 0022347613009517Nurul Khairiyah AmriAinda não há avaliações
- Pacifier and Bottle Nipples: The Targets For Poor Breastfeeding OutcomesDocumento3 páginasPacifier and Bottle Nipples: The Targets For Poor Breastfeeding Outcomesbeleg100% (1)
- Breastfeeding and The Use of Human Milk 2005Documento13 páginasBreastfeeding and The Use of Human Milk 2005Juan Pablo Anabalón SaavedraAinda não há avaliações
- PCH 35 01 014 PDFDocumento10 páginasPCH 35 01 014 PDFDhika Adhi PratamaAinda não há avaliações
- JACI 2010 Can Early Introduction of Egg Prevent Egg Allergy in Infants A Population-Based Study PDFDocumento7 páginasJACI 2010 Can Early Introduction of Egg Prevent Egg Allergy in Infants A Population-Based Study PDFTri RachmadijantoAinda não há avaliações
- NIH Public Access: Author ManuscriptDocumento9 páginasNIH Public Access: Author ManuscriptmcndAinda não há avaliações
- Growth of Infants Fed Formula With Evolving Nutrition CompositionDocumento13 páginasGrowth of Infants Fed Formula With Evolving Nutrition CompositionJohn JAinda não há avaliações
- Current Recommendations in Preterm Infants? Postnatal Malnutrition and Growth Retardation: An Inevitable Consequence ofDocumento6 páginasCurrent Recommendations in Preterm Infants? Postnatal Malnutrition and Growth Retardation: An Inevitable Consequence ofrafikrAinda não há avaliações
- Bowling Nur 4222 Integrated Review FinalDocumento14 páginasBowling Nur 4222 Integrated Review Finalapi-349455792Ainda não há avaliações
- Clinical Pediatrics: Postdischarge Feeding Patterns in Early-And Late-Preterm InfantsDocumento7 páginasClinical Pediatrics: Postdischarge Feeding Patterns in Early-And Late-Preterm InfantsCleoanne GallegosAinda não há avaliações
- Timing of Solid Food Introduction and Association With Later Childhood Overweight and Obesity: The IDEFICS StudyDocumento8 páginasTiming of Solid Food Introduction and Association With Later Childhood Overweight and Obesity: The IDEFICS Studytania toroAinda não há avaliações
- Randomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesDocumento9 páginasRandomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesSardono WidinugrohoAinda não há avaliações
- Neonatalnutrition: Scott C. DenneDocumento12 páginasNeonatalnutrition: Scott C. DenneSugiantoAinda não há avaliações
- The Relationship Between Feeding Practices and Children Ages 0-24monthsDocumento42 páginasThe Relationship Between Feeding Practices and Children Ages 0-24monthsGiovanni MartinAinda não há avaliações
- Intravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Documento5 páginasIntravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Wira Sasmita P100% (1)
- Laboratory Diagnosis of Bacterial Gastroenteritis: Romney M. Humphries, Andrea J. LinscottDocumento29 páginasLaboratory Diagnosis of Bacterial Gastroenteritis: Romney M. Humphries, Andrea J. LinscottFatah Jati PAinda não há avaliações
- Woodell2018 (Jurnal Asli)Documento13 páginasWoodell2018 (Jurnal Asli)Fatah Jati PAinda não há avaliações
- Tissue Factor: An Essential Mediator of Hemostasis and Trigger of ThrombosisDocumento19 páginasTissue Factor: An Essential Mediator of Hemostasis and Trigger of ThrombosisFatah Jati PAinda não há avaliações
- Ambroxol PDFDocumento45 páginasAmbroxol PDFFatah Jati PAinda não há avaliações
- Pemba Has AnDocumento15 páginasPemba Has AnFatah Jati PAinda não há avaliações
- Exclusive Breastfeeding Reduces Necrotizing Enterocolitis in Premature InfantsDocumento2 páginasExclusive Breastfeeding Reduces Necrotizing Enterocolitis in Premature InfantsFatah Jati PAinda não há avaliações
- Curcuma Longa As Medicinal Herb in The TreatmentDocumento8 páginasCurcuma Longa As Medicinal Herb in The TreatmentFatah Jati PAinda não há avaliações
- Jurnal CochraneDocumento96 páginasJurnal CochraneFatah Jati PAinda não há avaliações
- 3159191445028100466Documento1 página3159191445028100466Fatah Jati PAinda não há avaliações
- Curcuma Longa As Medicinal Herb in The TreatmentDocumento8 páginasCurcuma Longa As Medicinal Herb in The TreatmentFatah Jati PAinda não há avaliações
- Food Allergy Prevention and Treatment - Cow's Milk AllergyDocumento19 páginasFood Allergy Prevention and Treatment - Cow's Milk AllergyPatrick nyawiraAinda não há avaliações
- Health QatarDocumento58 páginasHealth QatarDuilio GuerreroAinda não há avaliações
- Immediate Newborn Care: Care of The Newborn at The Time of BirthDocumento42 páginasImmediate Newborn Care: Care of The Newborn at The Time of BirthDara Gi's FashionHausAinda não há avaliações
- Baby Food in Vietnam AnalysisDocumento3 páginasBaby Food in Vietnam AnalysisAbdcAinda não há avaliações
- Bsc. Nursing Examination: Revision QuestionsDocumento79 páginasBsc. Nursing Examination: Revision QuestionsNixi MbuthiaAinda não há avaliações
- Need of New Born and Parenting ProcessDocumento13 páginasNeed of New Born and Parenting ProcessKrini TandelAinda não há avaliações
- MIDTERMS EXAM-NutriLECDocumento9 páginasMIDTERMS EXAM-NutriLECNelia AlfonsoAinda não há avaliações
- Epilepsy in PregnancyDocumento33 páginasEpilepsy in PregnancyxxdrivexxAinda não há avaliações
- Referral Letter Paragraph StructureDocumento5 páginasReferral Letter Paragraph StructureJayson Dela Torre CortesAinda não há avaliações
- Approved MICS Balochistan Final Report 23 November 2011 PDFDocumento318 páginasApproved MICS Balochistan Final Report 23 November 2011 PDFAkhtar RashidAinda não há avaliações
- Essential Infant Nutrition: Benefits of Exclusive BreastfeedingDocumento11 páginasEssential Infant Nutrition: Benefits of Exclusive BreastfeedingRosa PalconitAinda não há avaliações
- Essential Immediate Newborn CareDocumento33 páginasEssential Immediate Newborn CareShenaAinda não há avaliações
- NCM 107 RLE Concept of Essential Intrapartum and Newborn CareDocumento15 páginasNCM 107 RLE Concept of Essential Intrapartum and Newborn CareFranz goAinda não há avaliações
- Benefits of Rooming-In for Mothers and BabiesDocumento3 páginasBenefits of Rooming-In for Mothers and BabiesAlisha Buyungan MundocAinda não há avaliações
- Lorma Colleges Patient Health History Related Learning ExperienceDocumento2 páginasLorma Colleges Patient Health History Related Learning Experienceivy annAinda não há avaliações
- استبيان سوء التغذية جامعة عمرانDocumento7 páginasاستبيان سوء التغذية جامعة عمرانAkram ZayedAinda não há avaliações
- WHO Guidlines For Manganese 2021Documento68 páginasWHO Guidlines For Manganese 2021Pike TVAinda não há avaliações
- Kangroo Mother Care PDFDocumento25 páginasKangroo Mother Care PDFMission Neet-PgAinda não há avaliações
- Provide Care and Support To ChildrenDocumento12 páginasProvide Care and Support To ChildrenGie Apilado Ranay67% (3)
- Nutrition During The Life CycleDocumento335 páginasNutrition During The Life Cycleapi-19916399100% (2)
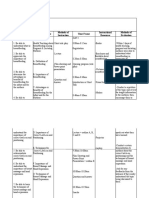
- Learning Objectives Content Outline Methods of Instruction Time Frame Instructional Resources Methods of EvaluationDocumento3 páginasLearning Objectives Content Outline Methods of Instruction Time Frame Instructional Resources Methods of EvaluationteuuuuAinda não há avaliações
- Meera Devi - A Parivartan Self-Help Group MemberDocumento2 páginasMeera Devi - A Parivartan Self-Help Group MemberS_digitalGREENAinda não há avaliações
- Penggunaan Kontrasepsi Hormonal Dan Produksi Air SDocumento6 páginasPenggunaan Kontrasepsi Hormonal Dan Produksi Air SFanny TifannyAinda não há avaliações
- Chapter 1-3 ThesisDocumento20 páginasChapter 1-3 ThesisMarianne Gonzales100% (1)
- Module 3 Hierarchical Relationship of Policy, Plan, Program, Project and ActivityDocumento2 páginasModule 3 Hierarchical Relationship of Policy, Plan, Program, Project and ActivityClaire GargaritaAinda não há avaliações
- Internet Resource AssignmentDocumento5 páginasInternet Resource Assignmentapi-220161595Ainda não há avaliações
- Basic breastfeeding positions and latch-on techniquesDocumento5 páginasBasic breastfeeding positions and latch-on techniquesInes Camilla PutriAinda não há avaliações
- Essential Intrapartum and Newborn Care (EINC)Documento26 páginasEssential Intrapartum and Newborn Care (EINC)Julianne B. Dela CruzAinda não há avaliações
- Formulations For Fortified Complementary Foods and Supplements: Review of Successful Products For Improving The Nutritional Status of Infants and Young ChildrenDocumento17 páginasFormulations For Fortified Complementary Foods and Supplements: Review of Successful Products For Improving The Nutritional Status of Infants and Young ChildrenDinesh SenathipathiAinda não há avaliações
- Assignment On Drugs Used For NewbornDocumento11 páginasAssignment On Drugs Used For Newbornvarshasharma05100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 5 de 5 estrelas5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (169)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsAinda não há avaliações
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementNo EverandTechniques Exercises And Tricks For Memory ImprovementNota: 4.5 de 5 estrelas4.5/5 (40)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisNo EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisNota: 3.5 de 5 estrelas3.5/5 (130)
- The Ultimate Guide To Memory Improvement TechniquesNo EverandThe Ultimate Guide To Memory Improvement TechniquesNota: 5 de 5 estrelas5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 5 de 5 estrelas5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (327)
- Troubled: A Memoir of Foster Care, Family, and Social ClassNo EverandTroubled: A Memoir of Foster Care, Family, and Social ClassNota: 5 de 5 estrelas5/5 (21)
- The Happiness Trap: How to Stop Struggling and Start LivingNo EverandThe Happiness Trap: How to Stop Struggling and Start LivingNota: 4 de 5 estrelas4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 3.5 de 5 estrelas3.5/5 (31)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsAinda não há avaliações
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNo EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNota: 5 de 5 estrelas5/5 (3)