Você também pode gostar
- Hira Ratan Manek. Solarhealing. Sun GazingDocumento15 páginasHira Ratan Manek. Solarhealing. Sun GazingEduardo Furihata100% (2)
- ZA Zung Anxiety ScaleDocumento1 páginaZA Zung Anxiety ScaleKomala SariAinda não há avaliações
- Fitzpatrick Skin Type Classification ScaleDocumento3 páginasFitzpatrick Skin Type Classification ScaleHanarisha Putri AzkiaAinda não há avaliações
- Assessment of The Efficacy and Tolerance of A New Combination of Retinoids and Depigmenting Agents in The Treatment of MelasmaDocumento8 páginasAssessment of The Efficacy and Tolerance of A New Combination of Retinoids and Depigmenting Agents in The Treatment of MelasmaAna Karina Alvarado OsorioAinda não há avaliações
- Oral Tranexamic Acid For The Treatment of MelasmaDocumento12 páginasOral Tranexamic Acid For The Treatment of MelasmaBeatriz CristinaAinda não há avaliações
- 05-BoNtA 568Documento44 páginas05-BoNtA 568Yovie Prayekti100% (2)
- Sothys, The Professional DifferenceDocumento29 páginasSothys, The Professional DifferenceNazihCosmeticsAinda não há avaliações
- Maintain Good Health as a Pilot: A Guide to Fitness to FlyDocumento22 páginasMaintain Good Health as a Pilot: A Guide to Fitness to FlyR. LoboAinda não há avaliações
- Spring Break ChemistryDocumento2 páginasSpring Break Chemistryapi-213793181Ainda não há avaliações
- EWG's 2010 Sunscreen GuideDocumento54 páginasEWG's 2010 Sunscreen GuideEnvironmental Working GroupAinda não há avaliações
- Oral Antibiotic Therapy For Acne Vulgaris PDFDocumento8 páginasOral Antibiotic Therapy For Acne Vulgaris PDFEka Sulistyowati PAinda não há avaliações
- 3 Eye Irritation enDocumento76 páginas3 Eye Irritation enEvelyng Taype Espinoza100% (1)
- Keratinocyte Exosomes Modulate Melanocyte PigmentationDocumento8 páginasKeratinocyte Exosomes Modulate Melanocyte Pigmentationluck2livAinda não há avaliações
- Basic Principles of Wound ManagementDocumento14 páginasBasic Principles of Wound ManagementLuis RuizAinda não há avaliações
- A Novel Approach Transdermal GelDocumento10 páginasA Novel Approach Transdermal GelTira MaharaniAinda não há avaliações
- Risk Factors of Gastritis and Its Prevalence Among Patients Visiting Kalkaal Hospital, Mogadishu, SomaliaDocumento6 páginasRisk Factors of Gastritis and Its Prevalence Among Patients Visiting Kalkaal Hospital, Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- DON'T BE LEFT IN THE DARK: LEARN HOW TO MASTER CHEMICAL PEELS and MORE... for a world of diverse skin tonesNo EverandDON'T BE LEFT IN THE DARK: LEARN HOW TO MASTER CHEMICAL PEELS and MORE... for a world of diverse skin tonesNota: 5 de 5 estrelas5/5 (1)
- Standards For Non-Surgical Cosmetic Procedures PDFDocumento18 páginasStandards For Non-Surgical Cosmetic Procedures PDFgourav jainAinda não há avaliações
- Geriatric DermatologyDocumento30 páginasGeriatric DermatologyMudsa Iing IletoAinda não há avaliações
- Pigmentary Disorders ExplainedDocumento40 páginasPigmentary Disorders ExplainedCHALIE MEQU100% (1)
- Presentación Gama Mesohyal - en v1.1Documento26 páginasPresentación Gama Mesohyal - en v1.1Niculae Bogdan DimitrieAinda não há avaliações
- 10 1097@DSS 0000000000001281Documento11 páginas10 1097@DSS 0000000000001281plastic guardiansAinda não há avaliações
- Peeling and Microdermabrasion Changes HystologicalsDocumento6 páginasPeeling and Microdermabrasion Changes HystologicalsBrian MacíaAinda não há avaliações
- Guidelines on Aesthetic Medical PracticeDocumento47 páginasGuidelines on Aesthetic Medical Practicezahisma890% (1)
- Ulthera Facial Tightening Without SurgeryDocumento3 páginasUlthera Facial Tightening Without SurgeryChaojaAinda não há avaliações
- 7 Active Ingredients For Special Products: 7.1 Definition of Special CreamsDocumento43 páginas7 Active Ingredients For Special Products: 7.1 Definition of Special CreamsElizabeth TovittoAinda não há avaliações
- 2.DR - SILVI.Structural Approach To Aesthetic RejuvenationDocumento18 páginas2.DR - SILVI.Structural Approach To Aesthetic RejuvenationResty Agiastuty Eka PutriAinda não há avaliações
- AR 005 2021 Formulation Peptides ProteinsDocumento12 páginasAR 005 2021 Formulation Peptides ProteinsKaif KhanAinda não há avaliações
- The Art of Chemical PeelingDocumento5 páginasThe Art of Chemical PeelingBrian MacíaAinda não há avaliações
- Chemical Peels Deep, Medium, and LightDocumento9 páginasChemical Peels Deep, Medium, and LightDeborah DobieszAinda não há avaliações
- Chemical Peels in The Treatment of Acne PDFDocumento8 páginasChemical Peels in The Treatment of Acne PDFSpica AdharaAinda não há avaliações
- Dermatological and Transdermal FormulationsDocumento578 páginasDermatological and Transdermal FormulationsEdgardo Ed Ramirez50% (2)
- Harmful Carcinogenic Ingredients in Skin CareDocumento3 páginasHarmful Carcinogenic Ingredients in Skin CareDisha T100% (1)
- Health Care in AustraliaDocumento6 páginasHealth Care in AustraliaNeil MenezesAinda não há avaliações
- Disorders of Pigmentation 1Documento56 páginasDisorders of Pigmentation 1Ahmed Noureldin AhmedAinda não há avaliações
- Journal of The American Academy of Dermatology Volume 77 Issue 4 2017 (Doi 10.1016 - J.jaad.2017.01.036) Chaowattanapanit, Suteeraporn Silpa-Archa, Narumol Kohli, Inde - Postinflammatory HyperpigmeDocumento15 páginasJournal of The American Academy of Dermatology Volume 77 Issue 4 2017 (Doi 10.1016 - J.jaad.2017.01.036) Chaowattanapanit, Suteeraporn Silpa-Archa, Narumol Kohli, Inde - Postinflammatory HyperpigmedikativiAinda não há avaliações
- CHAPTER 4 Helping Patients With Adherence and Decision Making CommskillsDocumento5 páginasCHAPTER 4 Helping Patients With Adherence and Decision Making CommskillsKacie YsulatAinda não há avaliações
- Medicinal Chemistry of Antihelmentics: Kim J.BDocumento25 páginasMedicinal Chemistry of Antihelmentics: Kim J.BprecyAinda não há avaliações
- Skin Pigmentation + Hari DisorderDocumento113 páginasSkin Pigmentation + Hari DisorderAfiqah So JasmiAinda não há avaliações
- Essay GMODocumento3 páginasEssay GMOFrank AnguetaAinda não há avaliações
- Treating MelasmaDocumento7 páginasTreating MelasmaPrabhat BhatAinda não há avaliações
- Botox - Full - ChapterDocumento21 páginasBotox - Full - ChapterkatityAinda não há avaliações
- Compounding (I)Documento90 páginasCompounding (I)Tantri RaraAinda não há avaliações
- Glycolic Acid Peel Therapy - A Current ReviewDocumento8 páginasGlycolic Acid Peel Therapy - A Current ReviewElaine MedeirosAinda não há avaliações
- FDA Regulation of HIFU DevicesDocumento7 páginasFDA Regulation of HIFU DevicesFadly HawariAinda não há avaliações
- Keloid: OccurrenceDocumento4 páginasKeloid: OccurrenceHendy MasjayantoAinda não há avaliações
- Plasma For Facial Rejuvenation 10.1111@jocd.12876Documento9 páginasPlasma For Facial Rejuvenation 10.1111@jocd.12876Lorena AcevedoAinda não há avaliações
- Occupational Medicine OverviewDocumento41 páginasOccupational Medicine OverviewVickas GopeeAinda não há avaliações
- Mesotherapy by Institute BCN EnesfrDocumento32 páginasMesotherapy by Institute BCN Enesfrmarketing4558Ainda não há avaliações
- You Ought To KnowDocumento18 páginasYou Ought To KnowpradeeporissaAinda não há avaliações
- Skin Capacitance Imaging: A Non-Optical Method for Assessing Skin Surface FeaturesDocumento160 páginasSkin Capacitance Imaging: A Non-Optical Method for Assessing Skin Surface Featuresidham khalidAinda não há avaliações
- Overview of Skin Aging and PhotoagingDocumento7 páginasOverview of Skin Aging and PhotoagingtissanAinda não há avaliações
- Ottawa Charter For Health PromotionDocumento3 páginasOttawa Charter For Health PromotiontataAinda não há avaliações
- Notes of Guidance of Cosmetic Safety Evaluation 9 EdDocumento151 páginasNotes of Guidance of Cosmetic Safety Evaluation 9 EdalexAinda não há avaliações
- Sytenol A Brochure Acne 2016Documento8 páginasSytenol A Brochure Acne 2016dian kaizenAinda não há avaliações
- MelasmaDocumento20 páginasMelasmaiyankRian100% (1)
- Psoriasis Comorbidities ReviewDocumento8 páginasPsoriasis Comorbidities ReviewIvanWinardyAinda não há avaliações
- Oxidation of Amino Acids, Peptides, and Proteins: Kinetics and MechanismNo EverandOxidation of Amino Acids, Peptides, and Proteins: Kinetics and MechanismAinda não há avaliações
- Study Alliance Guideline On The Management of Acne in South East AsiaDocumento9 páginasStudy Alliance Guideline On The Management of Acne in South East AsiaaldiraaAinda não há avaliações
- Causes and Effects of Acne on Teenagers' Self-Esteem and Social LivesDocumento16 páginasCauses and Effects of Acne on Teenagers' Self-Esteem and Social LivesLemuel KimAinda não há avaliações
- Skin Aging and Its TreatmentDocumento12 páginasSkin Aging and Its TreatmentViola Arsita ErrendyarAinda não há avaliações
- Skincare, The Beginners Guide to Good Skincare HabitsNo EverandSkincare, The Beginners Guide to Good Skincare HabitsAinda não há avaliações
- Injection Techniques For Midface Volumization UsinDocumento9 páginasInjection Techniques For Midface Volumization UsinAnjana Rukmani100% (1)
- Topical Products For The Aging Face: Clinics in Plastic Surgery May 2016Documento9 páginasTopical Products For The Aging Face: Clinics in Plastic Surgery May 2016valentina de jesus zuniga barrosAinda não há avaliações
- Peran Trombosit Pada Proses InflamasiDocumento14 páginasPeran Trombosit Pada Proses InflamasimonitamiftahAinda não há avaliações
- Asam Traneksamat Untuk KulitDocumento2 páginasAsam Traneksamat Untuk KulitmonitamiftahAinda não há avaliações
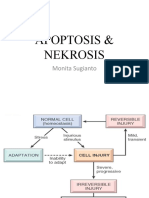
- Apoptosis & NekrosisDocumento13 páginasApoptosis & NekrosismonitamiftahAinda não há avaliações
- Apoptosis & NekrosisDocumento13 páginasApoptosis & NekrosismonitamiftahAinda não há avaliações
- LaserDocumento104 páginasLasermonitamiftah100% (1)
- Social Anxiety Screening ToolDocumento5 páginasSocial Anxiety Screening ToolKurt CutayAinda não há avaliações
- Lavees Cosmedics: Cara PakaiDocumento2 páginasLavees Cosmedics: Cara PakaimonitamiftahAinda não há avaliações
- Study Alliance Guideline On The Management of Acne in South East AsiaDocumento9 páginasStudy Alliance Guideline On The Management of Acne in South East AsiaaldiraaAinda não há avaliações
- Hakozaki 2002Documento12 páginasHakozaki 2002monitamiftahAinda não há avaliações
- Oral Collagen Supplementation For Skin Aging: A Fad or The Future?Documento3 páginasOral Collagen Supplementation For Skin Aging: A Fad or The Future?monitamiftahAinda não há avaliações
- Menopause Seminar Reviews Symptoms and TreatmentsDocumento11 páginasMenopause Seminar Reviews Symptoms and TreatmentsmonitamiftahAinda não há avaliações
- Oral Collagen Supplementation For Skin Aging: A Fad or The Future?Documento3 páginasOral Collagen Supplementation For Skin Aging: A Fad or The Future?monitamiftahAinda não há avaliações
- Generalized Anxiety Disorder (GAD) Screening ToolDocumento2 páginasGeneralized Anxiety Disorder (GAD) Screening ToolBrasa Y. de AlmiraAinda não há avaliações
- 5 e 68 D 1 A 893568Documento6 páginas5 e 68 D 1 A 893568monitamiftahAinda não há avaliações
- Asam Traneksamat Untuk KulitDocumento2 páginasAsam Traneksamat Untuk KulitmonitamiftahAinda não há avaliações
- Biologi MelanositDocumento17 páginasBiologi MelanositmonitamiftahAinda não há avaliações
- Biologi MelanositDocumento17 páginasBiologi MelanositmonitamiftahAinda não há avaliações
- Lehninger Principles of Biochemistry PDFDocumento37 páginasLehninger Principles of Biochemistry PDFmonitamiftahAinda não há avaliações
- Efek Immunologi Radiasi Sinar UV MatahariDocumento16 páginasEfek Immunologi Radiasi Sinar UV MataharimonitamiftahAinda não há avaliações
- Barkan - 2007 - Growth Hormone As An Anti-Aging Therapy - Do The Benefits Outweigh The RisksDocumento2 páginasBarkan - 2007 - Growth Hormone As An Anti-Aging Therapy - Do The Benefits Outweigh The RisksmonitamiftahAinda não há avaliações
- Lehninger Principles of Biochemistry PDFDocumento37 páginasLehninger Principles of Biochemistry PDFmonitamiftahAinda não há avaliações
- Peran Trombosit Pada Proses InflamasiDocumento14 páginasPeran Trombosit Pada Proses InflamasimonitamiftahAinda não há avaliações
- Peran Trombosit Pada Proses InflamasiDocumento14 páginasPeran Trombosit Pada Proses InflamasimonitamiftahAinda não há avaliações
- Guidelines Acne Vulgaris PDFDocumento14 páginasGuidelines Acne Vulgaris PDFmonitamiftahAinda não há avaliações
- International Journal of Dermatology Perempuan 1Documento16 páginasInternational Journal of Dermatology Perempuan 1monitamiftahAinda não há avaliações
- Management of Aging SkinDocumento19 páginasManagement of Aging SkinmonitamiftahAinda não há avaliações
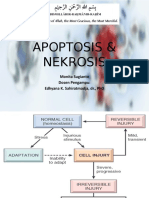
- Apoptosis & Nekrosis: Monita Sugianto Dosen Pengampu: Edhyana K. Sahiratmadja, DR., PHDDocumento34 páginasApoptosis & Nekrosis: Monita Sugianto Dosen Pengampu: Edhyana K. Sahiratmadja, DR., PHDmonitamiftahAinda não há avaliações
- Apoptosis & Nekrosis: Monita Sugianto Dosen Pengampu: Edhyana K. Sahiratmadja, DR., PHDDocumento34 páginasApoptosis & Nekrosis: Monita Sugianto Dosen Pengampu: Edhyana K. Sahiratmadja, DR., PHDmonitamiftahAinda não há avaliações
- BOE Sets Goals For Next Year: Haddonfield Tops Collingswood, 10-0Documento24 páginasBOE Sets Goals For Next Year: Haddonfield Tops Collingswood, 10-0elauwitAinda não há avaliações
- Review: Stephan Lautenschlager, Hans Christian Wulf, Mark R PittelkowDocumento10 páginasReview: Stephan Lautenschlager, Hans Christian Wulf, Mark R PittelkowHernan Antonio Cardozo TorresAinda não há avaliações
- CONNECTED: Canadian Cancer Society, Ontario Division - Impact Report 2008-2009Documento40 páginasCONNECTED: Canadian Cancer Society, Ontario Division - Impact Report 2008-2009canadiancancersocietyAinda não há avaliações
- Penetapan Potensi Tabir Surya Krim Ekstrak Etanol Daun Ceremai (PhyllanthusDocumento7 páginasPenetapan Potensi Tabir Surya Krim Ekstrak Etanol Daun Ceremai (Phyllanthuspurity sabilaAinda não há avaliações
- Yoga Journal - January 2014 AUDocumento116 páginasYoga Journal - January 2014 AUarash.moo.savi100% (1)
- MODULE-1 Unit1Documento11 páginasMODULE-1 Unit1Poison PinkAinda não há avaliações
- Current Concepts in Plastic Surgery - AgulloDocumento273 páginasCurrent Concepts in Plastic Surgery - AgulloAnonymous LnWIBo1GAinda não há avaliações
- Bad & BSF Sunscreen Fact SheetDocumento9 páginasBad & BSF Sunscreen Fact SheetArkadiyAinda não há avaliações
- Skin Pigmentation and Associated Diseases in KsaDocumento6 páginasSkin Pigmentation and Associated Diseases in KsaIJAR JOURNALAinda não há avaliações
- Asia On TourDocumento378 páginasAsia On TourJohn SandersAinda não há avaliações
- Photoprotection: Part I. Photoprotection by Naturally Occurring, Physical, and Systemic AgentsDocumento12 páginasPhotoprotection: Part I. Photoprotection by Naturally Occurring, Physical, and Systemic AgentsThaís SagratzhiAinda não há avaliações
- Manuale Prestige 1100Documento114 páginasManuale Prestige 1100Paulmanke100% (10)
- MelanoBronze Stimulation of Melanin Synthesis For Tanning and Protection SOFW 2006 PDFDocumento5 páginasMelanoBronze Stimulation of Melanin Synthesis For Tanning and Protection SOFW 2006 PDFTony Abott100% (1)
- Consent For Laser Hair RemovalDocumento2 páginasConsent For Laser Hair RemovalCassi CrumAinda não há avaliações
- The Fitzpatrick Skin Type ChartDocumento2 páginasThe Fitzpatrick Skin Type ChartLuis Fernando Sabogal FrancoAinda não há avaliações
- Importance of Using SunscreenDocumento1 páginaImportance of Using SunscreenANNISA FITRIANIAinda não há avaliações
- Vitamin D MiraclesDocumento20 páginasVitamin D MiraclesDIN08Ainda não há avaliações
- Skin Health Teaching GuideDocumento7 páginasSkin Health Teaching GuideSandy HernandezAinda não há avaliações
- KBL 7000 Owners ManualDocumento22 páginasKBL 7000 Owners ManualPaulmankeAinda não há avaliações
- Uma Kita.: Skylite Musicals 2019 Visual AtmosphereDocumento14 páginasUma Kita.: Skylite Musicals 2019 Visual AtmosphereJasmine AyuAinda não há avaliações
- Manuale Operativo Esprit 770Documento116 páginasManuale Operativo Esprit 770PaulmankeAinda não há avaliações
- Natural HygieneDocumento46 páginasNatural HygieneRyan Ricketts100% (2)
- המורת רדא עשת א " ד 1st February 2014: The Basic Premise of Tzoveya Temporary ColouringDocumento2 páginasהמורת רדא עשת א " ד 1st February 2014: The Basic Premise of Tzoveya Temporary ColouringLivingTorahAinda não há avaliações
- Sothys Product BrochureDocumento27 páginasSothys Product BrochureNazihCosmeticsAinda não há avaliações
- Lumea: BRI959, BRI956, BRI954, BRI953, BRI950Documento139 páginasLumea: BRI959, BRI956, BRI954, BRI953, BRI950libarmonicaAinda não há avaliações