Você também pode gostar
- Simultaneous Papillary Carcinoma in Thyroglossal Duct Cyst and ThyroidDocumento5 páginasSimultaneous Papillary Carcinoma in Thyroglossal Duct Cyst and ThyroidOncologiaGonzalezBrenes Gonzalez BrenesAinda não há avaliações
- Thyroglossal Duct Cyst StudyDocumento7 páginasThyroglossal Duct Cyst StudyAurel OctavianAinda não há avaliações
- Mangement of Thyroglossal Duct CystDocumento3 páginasMangement of Thyroglossal Duct CystmohamedhazemelfollAinda não há avaliações
- Medip, IJRMS-7729 ODocumento7 páginasMedip, IJRMS-7729 ORagupathi MAinda não há avaliações
- Burud 2020Documento8 páginasBurud 2020Wirda Elya SariAinda não há avaliações
- Jcem 0458Documento8 páginasJcem 0458abigailAinda não há avaliações
- 10 1097@scs 0000000000003278Documento3 páginas10 1097@scs 0000000000003278Meva'a RogerAinda não há avaliações
- Testicular Torsion: An Analysis of Sixteen Consecutive Cases and A Review of The LiteratureDocumento3 páginasTesticular Torsion: An Analysis of Sixteen Consecutive Cases and A Review of The LiteratureLea Bali Ulina SinurayaAinda não há avaliações
- Role of CT Scan in Diagnosis and Management of Otogenic Intracranial AbscessDocumento5 páginasRole of CT Scan in Diagnosis and Management of Otogenic Intracranial AbscessayundariprimaraniAinda não há avaliações
- Management of Thyroglossal Duct Cyst PDocumento3 páginasManagement of Thyroglossal Duct Cyst Pnugroho2212Ainda não há avaliações
- ANZ Journal of Surgery - 2021 - Wong - Cancer in Thyroglossal Duct CystsDocumento6 páginasANZ Journal of Surgery - 2021 - Wong - Cancer in Thyroglossal Duct CystsJamesLeeAinda não há avaliações
- Accepted Manuscript: 10.1016/j.jcms.2017.12.013Documento16 páginasAccepted Manuscript: 10.1016/j.jcms.2017.12.013stoia_sebiAinda não há avaliações
- Thyroglossal Duct Cyst & Sistrunk: A Case Series: July 2015Documento6 páginasThyroglossal Duct Cyst & Sistrunk: A Case Series: July 2015Victor Joel Rios GonzalesAinda não há avaliações
- Thyroid Isthmusectomy - A Critical AppraisalDocumento4 páginasThyroid Isthmusectomy - A Critical Appraisalentgo8282Ainda não há avaliações
- Chondrosarcoma of The Jaw: A Retrospective Series: ObjectivesDocumento6 páginasChondrosarcoma of The Jaw: A Retrospective Series: ObjectivesOMFS FKG UnimusAinda não há avaliações
- 1 s2.0 S0748798321001098 MainDocumento6 páginas1 s2.0 S0748798321001098 MainMihai MarinescuAinda não há avaliações
- Surgical management of elongated styloid process: intraoral or transcervical?Documento5 páginasSurgical management of elongated styloid process: intraoral or transcervical?kaluaxeniaAinda não há avaliações
- Thyroglossal Duct Cyst Carcinoma WithDocumento8 páginasThyroglossal Duct Cyst Carcinoma WithM Ali AdrianAinda não há avaliações
- Art 3Documento6 páginasArt 3Claudia IrimieAinda não há avaliações
- Minimal Hydrocelectomy Technique with ScrotoscopeDocumento6 páginasMinimal Hydrocelectomy Technique with ScrotoscopeAbdalsalaam AbraikAinda não há avaliações
- 60 TH Male Spermatic Cord HydroceleDocumento2 páginas60 TH Male Spermatic Cord HydroceleSofie HanafiahAinda não há avaliações
- Tuberculous Tenosynovitis as a Cause of Carpal Tunnel SyndromeDocumento3 páginasTuberculous Tenosynovitis as a Cause of Carpal Tunnel Syndromeshamim sheikhAinda não há avaliações
- 264 2011 Article 1480Documento6 páginas264 2011 Article 1480Paul Mendez AguilarAinda não há avaliações
- Recurrence Factors After Thyroglossal Duct Cyst SurgeryDocumento6 páginasRecurrence Factors After Thyroglossal Duct Cyst SurgeryKhairuman FitrahAinda não há avaliações
- Case Report: A Rare Case of Congenital Simple Cystic Ranula in A NeonateDocumento4 páginasCase Report: A Rare Case of Congenital Simple Cystic Ranula in A NeonateElvita Srie WahyuniAinda não há avaliações
- Thyroglossal Duct Cysts: Anatomy, Embryology and TreatmentDocumento7 páginasThyroglossal Duct Cysts: Anatomy, Embryology and TreatmentTasia RozakiahAinda não há avaliações
- 2018 Article 1362 PDFDocumento5 páginas2018 Article 1362 PDFAuliaMahdaniatiAinda não há avaliações
- Thoracoscopic Excision of Symptomatic Esophageal Duplication Cyst in Adult Population-Experience From A Tertiary Care CenterDocumento5 páginasThoracoscopic Excision of Symptomatic Esophageal Duplication Cyst in Adult Population-Experience From A Tertiary Care CenterIJAR JOURNALAinda não há avaliações
- Duktus ThyroglosusDocumento13 páginasDuktus ThyroglosusOscar BrooksAinda não há avaliações
- Testicular Torsion in Undescended TestisDocumento5 páginasTesticular Torsion in Undescended TestisjimAinda não há avaliações
- Referat Pleomorphic AdenomaDocumento6 páginasReferat Pleomorphic AdenomaAsrie Sukawatie PutrieAinda não há avaliações
- Medip, IJOHNS-388 ODocumento6 páginasMedip, IJOHNS-388 Onaveed gulAinda não há avaliações
- Clinicopathological Study of Thyroglossal Cyst 2j3c1n18asDocumento5 páginasClinicopathological Study of Thyroglossal Cyst 2j3c1n18asd202020315Ainda não há avaliações
- Successful Percutaneous Treatment of Extrahepatic Cystic Echinococcosis Through PAIR and Single Puncture Catheter TechniquesDocumento7 páginasSuccessful Percutaneous Treatment of Extrahepatic Cystic Echinococcosis Through PAIR and Single Puncture Catheter TechniquesSandu AlexandraAinda não há avaliações
- Diagnostic Accuracy Fine Needle Aspiration Cytology of Thyroid Gland LesionsDocumento6 páginasDiagnostic Accuracy Fine Needle Aspiration Cytology of Thyroid Gland LesionsinventionjournalsAinda não há avaliações
- f194 DikonversiDocumento5 páginasf194 DikonversiFarizka Dwinda HAinda não há avaliações
- International Journal of Surgery Case Reports: Case Report - Open AccessDocumento3 páginasInternational Journal of Surgery Case Reports: Case Report - Open AccesscagcmdAinda não há avaliações
- Laryngeal Chondrosarcoma of The Thyroid Cartilage: Case ReportDocumento5 páginasLaryngeal Chondrosarcoma of The Thyroid Cartilage: Case ReportelvirAinda não há avaliações
- Thyroglossal Duct Cyst in The Suprasternal RegionDocumento3 páginasThyroglossal Duct Cyst in The Suprasternal RegionKhairuman anandaAinda não há avaliações
- Wu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalDocumento4 páginasWu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalcharlaayasyafefiAinda não há avaliações
- Brain AbsesDocumento4 páginasBrain Absesmuthiadewi31Ainda não há avaliações
- Parathyroid Final PDFDocumento4 páginasParathyroid Final PDFgeoschorAinda não há avaliações
- Ectopic Cervical Thyroid Carcinoma-Review of The Literature With Illustrative Case SeriesDocumento8 páginasEctopic Cervical Thyroid Carcinoma-Review of The Literature With Illustrative Case SeriesAnonymous s4yarxAinda não há avaliações
- Clinical Neurology and Neurosurgery: SciencedirectDocumento7 páginasClinical Neurology and Neurosurgery: SciencedirectMella WarizkaAinda não há avaliações
- Cancer GuidelinesDocumento17 páginasCancer GuidelinesJoni WitziAinda não há avaliações
- Art 1Documento4 páginasArt 1Claudia IrimieAinda não há avaliações
- Indications For Thyroid Surgeryexperience of The Ent Departmentof Moulay Ismail Military Hospital in Meknes (About 103 Cases)Documento8 páginasIndications For Thyroid Surgeryexperience of The Ent Departmentof Moulay Ismail Military Hospital in Meknes (About 103 Cases)IJAR JOURNALAinda não há avaliações
- Niu 2019Documento7 páginasNiu 2019Dazz MiitAinda não há avaliações
- Indications of Ventriculoperitoneal Shunt: A Prospective StudyDocumento8 páginasIndications of Ventriculoperitoneal Shunt: A Prospective Studyvalencia suwardiAinda não há avaliações
- 45 Siddaganga EtalDocumento4 páginas45 Siddaganga EtaleditorijmrhsAinda não há avaliações
- 17-Potential Medicolegal RisksDocumento1 página17-Potential Medicolegal RisksSUSANAinda não há avaliações
- Delineation of de Quervain Tenosynovitis in Saudi Arabia and Literature ReviewDocumento6 páginasDelineation of de Quervain Tenosynovitis in Saudi Arabia and Literature ReviewIJAR JOURNALAinda não há avaliações
- Intrinsic Third Ventricular Craniopharyngiomas: Report On Six Cases and A Review of The LiteratureDocumento8 páginasIntrinsic Third Ventricular Craniopharyngiomas: Report On Six Cases and A Review of The LiteratureAmina GoharyAinda não há avaliações
- Comparing Tonsillectomy Techniques: Dissection vs. CoblationDocumento6 páginasComparing Tonsillectomy Techniques: Dissection vs. CoblationKadekWatyAinda não há avaliações
- International Journal of Surgery Case ReportsDocumento3 páginasInternational Journal of Surgery Case ReportsYipno Wanhar El MawardiAinda não há avaliações
- Short - and Long-Term Outcomes at A Single InstitutionDocumento7 páginasShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahAinda não há avaliações
- Leiomyoma of The Esophagus: Open Versus Thoracoscopic EnucleationDocumento5 páginasLeiomyoma of The Esophagus: Open Versus Thoracoscopic EnucleationYacine Tarik AizelAinda não há avaliações
- Schick2006 Treatment PDFDocumento7 páginasSchick2006 Treatment PDFRifqi FAinda não há avaliações
- Complications of Tonsillectomy, Adenoidectomy and Adenotonsillectomy in Chittagong Medical College HospitalDocumento4 páginasComplications of Tonsillectomy, Adenoidectomy and Adenotonsillectomy in Chittagong Medical College Hospitalnaufal12345Ainda não há avaliações
- Atlas of Parathyroid Imaging and PathologyNo EverandAtlas of Parathyroid Imaging and PathologyAlexander L. ShifrinAinda não há avaliações
- Jurnal AppendicitisDocumento10 páginasJurnal AppendicitisEwoJatmikoAinda não há avaliações
- AAFP - Evaluation of Acute Abdomen in AdultsDocumento8 páginasAAFP - Evaluation of Acute Abdomen in AdultsTe HineahuoneAinda não há avaliações
- Ductus Thyroglosus CystDocumento4 páginasDuctus Thyroglosus CystkancutpaulkadotAinda não há avaliações
- Thyroglossal Duct Cyst - More Than Just An Embryological RemnantDocumento4 páginasThyroglossal Duct Cyst - More Than Just An Embryological RemnantkancutpaulkadotAinda não há avaliações
- Undescended Testicle - Harvard HealthDocumento3 páginasUndescended Testicle - Harvard HealthkancutpaulkadotAinda não há avaliações
- Molecules 22 01259 PDFDocumento20 páginasMolecules 22 01259 PDFkancutpaulkadotAinda não há avaliações
- Gross HSB A - The Facial MusclesDocumento4 páginasGross HSB A - The Facial MusclesAngelo BautistaAinda não há avaliações
- Assignment 3Documento2 páginasAssignment 3Sophie Siti SAinda não há avaliações
- Protocols MSK MRI (2010)Documento123 páginasProtocols MSK MRI (2010)Danish218100% (1)
- 7 - Cholinomimetic DrugsDocumento50 páginas7 - Cholinomimetic DrugslalitrajindoliaAinda não há avaliações
- The Biologic Basis For Libido: James G. Pfaus, PHD, and Lisa A.Scepkowski, MaDocumento6 páginasThe Biologic Basis For Libido: James G. Pfaus, PHD, and Lisa A.Scepkowski, MaPaul AsturbiarisAinda não há avaliações
- The Midlife: Henrietta V. Cabado-Española, MD, FPPADocumento7 páginasThe Midlife: Henrietta V. Cabado-Española, MD, FPPADoc Prince CaballeroAinda não há avaliações
- Cell Culture PDFDocumento12 páginasCell Culture PDFSherwann Vergara Delos ReyesAinda não há avaliações
- Breast UltrasoundDocumento57 páginasBreast UltrasoundYoungFanjiensAinda não há avaliações
- 2011 - Melissa Hines - Gender Development and The Human BrainDocumento22 páginas2011 - Melissa Hines - Gender Development and The Human BrainDiego Alejandro Londoño CorreaAinda não há avaliações
- Anatomy Physiology The Endocrine System MCQ ExamDocumento37 páginasAnatomy Physiology The Endocrine System MCQ Examaminata6100% (4)
- Study Questions: CHAPTER 8 Microscopic Examination of Urine SedimentDocumento7 páginasStudy Questions: CHAPTER 8 Microscopic Examination of Urine SedimentTiara YantaAinda não há avaliações
- Procedures Used in The Management of DystociaDocumento17 páginasProcedures Used in The Management of DystociaVeterinary Online InstituteAinda não há avaliações
- Pathophysiology of Burn Injury (1) DVDocumento2 páginasPathophysiology of Burn Injury (1) DVRizzie Montes0% (1)
- NBDE Dental Boards Pedo 21 3Documento1 páginaNBDE Dental Boards Pedo 21 3NotoprosAinda não há avaliações
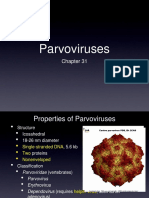
- Parvoviruses: Structure, Replication, DiseasesDocumento8 páginasParvoviruses: Structure, Replication, DiseasesAldila safitriAinda não há avaliações
- Pharmacology Case StudyDocumento4 páginasPharmacology Case StudyRichard S. RoxasAinda não há avaliações
- Complete Blood CountDocumento3 páginasComplete Blood CountivantototaeAinda não há avaliações
- Hemorrhage ShockDocumento17 páginasHemorrhage ShockgrizzlovAinda não há avaliações
- Reproductive Systems A. B. C. DDocumento6 páginasReproductive Systems A. B. C. DJamie BagundolAinda não há avaliações
- The Effectiveness of Makahiya (Mimosa Pudica) Leaves Extract As An Alternative Ovicide Against Dengue Mosquito (Aedes Aegypti) EggsDocumento6 páginasThe Effectiveness of Makahiya (Mimosa Pudica) Leaves Extract As An Alternative Ovicide Against Dengue Mosquito (Aedes Aegypti) EggsIya Necole GuimaryAinda não há avaliações
- Feng Shui Divination Qi Men Dun Jia From The Feng Shui InstituteDocumento7 páginasFeng Shui Divination Qi Men Dun Jia From The Feng Shui InstituteKiyanka Nastya100% (2)
- Antenatal Assessment FormatDocumento9 páginasAntenatal Assessment FormatVijith.V.kumar93% (14)
- Handling and care of experimental animalsDocumento26 páginasHandling and care of experimental animalsABHINABA GUPTAAinda não há avaliações
- Animal Welfare CourseDocumento42 páginasAnimal Welfare CourseDr-Rmz RabadiAinda não há avaliações
- Reproduction and Heredity NotesDocumento63 páginasReproduction and Heredity NotesmceldowneaAinda não há avaliações
- The Tamil Nadu Dr. M.G.R. Medical University, Chennai Regulations of The UniversityDocumento88 páginasThe Tamil Nadu Dr. M.G.R. Medical University, Chennai Regulations of The UniversityAjay IyerAinda não há avaliações
- Nelson Last Minute Pediatrics Guide Covers Key Developmental MilestonesDocumento392 páginasNelson Last Minute Pediatrics Guide Covers Key Developmental Milestonesjeyaprakash jayaramanAinda não há avaliações
- Homeostasis and Higher Brain FunctionsDocumento84 páginasHomeostasis and Higher Brain Functionsbodeadumitru9261Ainda não há avaliações
- Echolation: Echolation Is Recognized As A Method Utilized by A Variety of Aquatic, Nocturnal, and CaveDocumento9 páginasEcholation: Echolation Is Recognized As A Method Utilized by A Variety of Aquatic, Nocturnal, and CaveJaimin K PatelAinda não há avaliações
- AnemiaDocumento2 páginasAnemiadianaAinda não há avaliações