Você também pode gostar
- Attitude of Secondary School Teachers Towards The Use of ICT in Teaching Learning ProcessDocumento4 páginasAttitude of Secondary School Teachers Towards The Use of ICT in Teaching Learning ProcessAnonymous lPvvgiQjR100% (1)
- A Review On Facial Expression Recognition TechniquesDocumento8 páginasA Review On Facial Expression Recognition TechniquesAnonymous lPvvgiQjRAinda não há avaliações
- Sine Cosine Based Algorithm For Data ClusteringDocumento5 páginasSine Cosine Based Algorithm For Data ClusteringAnonymous lPvvgiQjRAinda não há avaliações
- VHDL Implementation of 128 Bit Pipelined Blowfish AlgorithmDocumento5 páginasVHDL Implementation of 128 Bit Pipelined Blowfish AlgorithmAnonymous lPvvgiQjRAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- 2013 Audi A5 Cabriolet s5 Cabriolet 8Documento16 páginas2013 Audi A5 Cabriolet s5 Cabriolet 8Adrio BianchiAinda não há avaliações
- Clinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants - UpToDateDocumento42 páginasClinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants - UpToDatedocjime9004Ainda não há avaliações
- CASE 721F TIER 4 WHEEL LOADER Operator's Manual PDFDocumento17 páginasCASE 721F TIER 4 WHEEL LOADER Operator's Manual PDFfjskedmmsme0% (4)
- WCC PSV PDFDocumento40 páginasWCC PSV PDFAlejandro RamelaAinda não há avaliações
- GeoSS Event Seminar 12 July 2012 - SlidesDocumento15 páginasGeoSS Event Seminar 12 July 2012 - SlidesNurmanda RamadhaniAinda não há avaliações
- Demolition/Removal Permit Application Form: Planning, Property and Development DepartmentDocumento3 páginasDemolition/Removal Permit Application Form: Planning, Property and Development DepartmentAl7amdlellahAinda não há avaliações
- W4. Grade 10 Health - Q1 - M4 - v2Documento22 páginasW4. Grade 10 Health - Q1 - M4 - v2Jesmael PantalunanAinda não há avaliações
- The Aging Brain: Course GuidebookDocumento126 páginasThe Aging Brain: Course GuidebookIsabel Cristina Jaramillo100% (2)
- Silage Sampling and AnalysisDocumento5 páginasSilage Sampling and AnalysisG_ASantosAinda não há avaliações
- Exam Questions: Exam Title: Chapter MEK 8Documento4 páginasExam Questions: Exam Title: Chapter MEK 8vishnu sharmaAinda não há avaliações
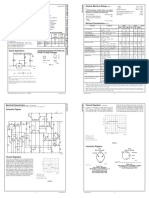
- LM 337Documento4 páginasLM 337matias robertAinda não há avaliações
- Krispy Kreme Doughnut Recipe - Immaculate BitesDocumento2 páginasKrispy Kreme Doughnut Recipe - Immaculate Bitesdaisydrops6Ainda não há avaliações
- BlahDocumento8 páginasBlahkwood84100% (1)
- 224 Chinese Healing ExercisesDocumento4 páginas224 Chinese Healing ExercisesKiné Therapeut-manuelle Masseur GabiAinda não há avaliações
- Material Rate PWD 2014...........Documento70 páginasMaterial Rate PWD 2014...........Shamsul IslamAinda não há avaliações
- Phoenix Contact DATA SHEETDocumento16 páginasPhoenix Contact DATA SHEETShivaniAinda não há avaliações
- 00516-CLIA-Newsletter Jan 06Documento4 páginas00516-CLIA-Newsletter Jan 06losangelesAinda não há avaliações
- Pure Vegeterian: Kousika (CaterersDocumento2 páginasPure Vegeterian: Kousika (CaterersShylender NagaAinda não há avaliações
- 1 PolarographyDocumento20 páginas1 PolarographyRiya Das100% (1)
- BRS PDFDocumento14 páginasBRS PDFGautam KhanwaniAinda não há avaliações
- Fawad Hussain, Feedback On Industrial Visit To Sahiwal Coal Power PlantDocumento2 páginasFawad Hussain, Feedback On Industrial Visit To Sahiwal Coal Power PlantSyed Fawad MarwatAinda não há avaliações
- Intimacy and Healthy Affective Maturaity - Fa-Winter09bDocumento9 páginasIntimacy and Healthy Affective Maturaity - Fa-Winter09bCarlos GiraldoAinda não há avaliações
- Martins Taylorb Os 10742 Final Opinion 2 11 2022 02898337xd2c78Documento9 páginasMartins Taylorb Os 10742 Final Opinion 2 11 2022 02898337xd2c78Live 5 NewsAinda não há avaliações
- Case Study LenovoDocumento10 páginasCase Study LenovoGOHAR GHAFFARAinda não há avaliações
- Rate Break Up 15500Documento1 páginaRate Break Up 15500Yash Raj Bhardwaj100% (1)
- Food Safety PosterDocumento1 páginaFood Safety PosterMP CariappaAinda não há avaliações
- Allison Weech Final ResumeDocumento1 páginaAllison Weech Final Resumeapi-506177291Ainda não há avaliações
- What Does She/He Look Like?: Height Build AGEDocumento18 páginasWhat Does She/He Look Like?: Height Build AGEHenrich Garcia LimaAinda não há avaliações
- J. Bleger ArtDocumento10 páginasJ. Bleger Artivancristina42Ainda não há avaliações
- CLSI Laboratory Documents Development and Control Approved Guideline NAT L COMM CLINICAL LAB STANDARDS 2006 PDFDocumento100 páginasCLSI Laboratory Documents Development and Control Approved Guideline NAT L COMM CLINICAL LAB STANDARDS 2006 PDFErvin RodriguezAinda não há avaliações