Você também pode gostar
- Ensure Your Documents Are Certified For Monash UniversityDocumento4 páginasEnsure Your Documents Are Certified For Monash UniversityDidikPrasetyoSuliAinda não há avaliações
- Review Article Role of Colors in Therapeutics Swami Gaurav: Volume: I: Issue-3: Nov-Dec - 2010Documento6 páginasReview Article Role of Colors in Therapeutics Swami Gaurav: Volume: I: Issue-3: Nov-Dec - 2010DidikPrasetyoSuliAinda não há avaliações
- Diagram Layang Final PostDocumento1 páginaDiagram Layang Final PostDidikPrasetyoSuliAinda não há avaliações
- 1 - 20 - 250Analisis-Perkembangan Terapi Leukemia Mieloid AkutDocumento18 páginas1 - 20 - 250Analisis-Perkembangan Terapi Leukemia Mieloid AkutDidikPrasetyoSuliAinda não há avaliações
- KuningDocumento36 páginasKuningRahmad SetiajiAinda não há avaliações
- Cheat Ffexvius11Documento78 páginasCheat Ffexvius11DidikPrasetyoSuliAinda não há avaliações
- Cheat Ffexvius11Documento78 páginasCheat Ffexvius11DidikPrasetyoSuliAinda não há avaliações
- s12966 014 0098 8.doc CompressedDocumento12 páginass12966 014 0098 8.doc CompressedDidikPrasetyoSuliAinda não há avaliações
- About Education in The UK: A. BackgroundDocumento3 páginasAbout Education in The UK: A. BackgroundDidikPrasetyoSuliAinda não há avaliações
- Judul JurnalDocumento1 páginaJudul JurnalDidikPrasetyoSuliAinda não há avaliações
- Sindrom Stevens JohnsonDocumento9 páginasSindrom Stevens JohnsonDidikPrasetyoSuli100% (1)
- SpeakingDocumento1 páginaSpeakingDidikPrasetyoSuliAinda não há avaliações
- A Prolonged State of Unconsciousness Is Known AsDocumento1 páginaA Prolonged State of Unconsciousness Is Known AsDidikPrasetyoSuliAinda não há avaliações
- Sindrom Stevens JohnsonDocumento9 páginasSindrom Stevens JohnsonDidikPrasetyoSuli100% (1)
- A Prolonged State of Unconsciousness Is Known AsDocumento1 páginaA Prolonged State of Unconsciousness Is Known AsDidikPrasetyoSuliAinda não há avaliações
- CHANGELOGDocumento1 páginaCHANGELOGDidikPrasetyoSuliAinda não há avaliações
- Dika Pung 3Documento9 páginasDika Pung 3DidikPrasetyoSuliAinda não há avaliações
- Benzathine Penicillin G For The Management of RHDDocumento8 páginasBenzathine Penicillin G For The Management of RHDDidikPrasetyoSuliAinda não há avaliações
- jpts-28-685 1Documento4 páginasjpts-28-685 1DidikPrasetyoSuliAinda não há avaliações
- SOX Trial Lancet Early Online VersionDocumento10 páginasSOX Trial Lancet Early Online VersionDidikPrasetyoSuliAinda não há avaliações
- SOX Trial Lancet Early Online VersionDocumento10 páginasSOX Trial Lancet Early Online VersionDidikPrasetyoSuliAinda não há avaliações
- Jurnal Vascular PDFDocumento6 páginasJurnal Vascular PDFRival Panca AnugrahAinda não há avaliações
- SOX Trial Lancet Early Online VersionDocumento10 páginasSOX Trial Lancet Early Online VersionDidikPrasetyoSuliAinda não há avaliações
- Cheat Ffexvius11Documento78 páginasCheat Ffexvius11DidikPrasetyoSuliAinda não há avaliações
- Describing WoundsDocumento4 páginasDescribing WoundsDidikPrasetyoSuliAinda não há avaliações
- Effect of Autogenic Relaxation Therapy on Acute Pain Levels in Abdominal Pain PatientsDocumento7 páginasEffect of Autogenic Relaxation Therapy on Acute Pain Levels in Abdominal Pain Patientsfathur0903Ainda não há avaliações
- Pen JaraDocumento12 páginasPen JaraDidikPrasetyoSuliAinda não há avaliações
- CPG On Dengue in Children 2017Documento108 páginasCPG On Dengue in Children 2017Hannah LeiAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Optimal Running Dose and Cardiovascular Risk: Raining Revention AND EhabilitationDocumento7 páginasOptimal Running Dose and Cardiovascular Risk: Raining Revention AND EhabilitationTiara SafitriAinda não há avaliações
- CT Cardiac Master IDocumento45 páginasCT Cardiac Master IAndreea RomanAinda não há avaliações
- CVPDocumento23 páginasCVPShalini KaluraAinda não há avaliações
- Jurnal Internasional Draft 3Documento8 páginasJurnal Internasional Draft 3thenytirtaAinda não há avaliações
- Hands On CPR WorksheetDocumento1 páginaHands On CPR Worksheetapi-404833978Ainda não há avaliações
- Anesthesia For Endovascular Aortic Repair - UpToDateDocumento48 páginasAnesthesia For Endovascular Aortic Repair - UpToDatematheusbbragacAinda não há avaliações
- Adrenergic Antagonist 2 (Propranolol)Documento5 páginasAdrenergic Antagonist 2 (Propranolol)ziad shahinAinda não há avaliações
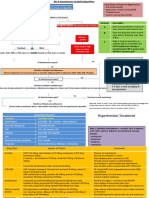
- Guideline HTDocumento61 páginasGuideline HTDwi PutrisariAinda não há avaliações
- Coronary Artery Disease (CAD) NCLEX QuestionsDocumento7 páginasCoronary Artery Disease (CAD) NCLEX QuestionsMelodia Turqueza GandezaAinda não há avaliações
- HF and CAD Case ScenarioDocumento4 páginasHF and CAD Case Scenariosandra M. CovarrubiasAinda não há avaliações
- ECG Guide: Understanding Waves, Intervals & Electrical EventsDocumento164 páginasECG Guide: Understanding Waves, Intervals & Electrical EventsMohsan RafiqAinda não há avaliações
- DR Oktalisa Letter For Poster Presentation Eurothrombosis Summit 2015Documento2 páginasDR Oktalisa Letter For Poster Presentation Eurothrombosis Summit 2015WennyAinda não há avaliações
- NU 636 WK 2 DP 2 - Treatment of HyperlipidemiaDocumento3 páginasNU 636 WK 2 DP 2 - Treatment of HyperlipidemiaShayAinda não há avaliações
- Principle of Aerobic ExercisesDocumento46 páginasPrinciple of Aerobic Exercisesway to satlok100% (1)
- Acsm (042 082)Documento41 páginasAcsm (042 082)김동현Ainda não há avaliações
- Acyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsDocumento17 páginasAcyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsAgustinaAinda não há avaliações
- Jugular Venous Pressure: It's Easier Than It LooksDocumento25 páginasJugular Venous Pressure: It's Easier Than It LooksManggarsari SdwqAinda não há avaliações
- Different Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled TrialDocumento8 páginasDifferent Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled Trialratnayanti udinAinda não há avaliações
- Nurses Need to Know About Stroke CareDocumento68 páginasNurses Need to Know About Stroke CareSuci Aning TAinda não há avaliações
- WelchAllyn PIC30,40,50 Defibrillator - Service Manual PDFDocumento289 páginasWelchAllyn PIC30,40,50 Defibrillator - Service Manual PDFandres2013bio100% (1)
- Monitoring-Form in PATH FITDocumento7 páginasMonitoring-Form in PATH FITSydsyd DawiliAinda não há avaliações
- Blood Vessels GuideDocumento40 páginasBlood Vessels Guidetas xoAinda não há avaliações
- Welch Allyn Home Hypertension Program Infographic PosterDocumento1 páginaWelch Allyn Home Hypertension Program Infographic PosterBerto YomoAinda não há avaliações
- Management of Acute Ischemic Stroke: Michael S Phipps, Carolyn A CroninDocumento15 páginasManagement of Acute Ischemic Stroke: Michael S Phipps, Carolyn A CroninPatty MArivel ReinosoAinda não há avaliações
- Profil Pemberian Nifedipine Kombinasi Metildopa Dan Mgso Pada Pasien Pre-Eklamsi Berat Di Rumah Sakit Daerah Mangusada BadungDocumento8 páginasProfil Pemberian Nifedipine Kombinasi Metildopa Dan Mgso Pada Pasien Pre-Eklamsi Berat Di Rumah Sakit Daerah Mangusada BadungPratama InsaniAinda não há avaliações
- CPR Cheat Sheet and Study GuideDocumento14 páginasCPR Cheat Sheet and Study GuideHenz Freeman0% (1)
- CASE PRESENTATION ON U AnginaDocumento40 páginasCASE PRESENTATION ON U AnginaSafoora RafeeqAinda não há avaliações
- Grade 9 Biology Lesson on the Circulatory SystemDocumento9 páginasGrade 9 Biology Lesson on the Circulatory SystemmicahxAinda não há avaliações
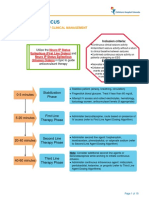
- JNC 8 Hypertension Guideline Algorithm CardDocumento2 páginasJNC 8 Hypertension Guideline Algorithm Cardismailuntung0% (1)
- Final Atcofliflozin Binder DiabetesDocumento23 páginasFinal Atcofliflozin Binder DiabetesEslamAinda não há avaliações