Você também pode gostar
- PeopleSoft HRMS Interview Questions, Answers, and ExplanationsNo EverandPeopleSoft HRMS Interview Questions, Answers, and ExplanationsNota: 4.5 de 5 estrelas4.5/5 (3)
- UAM UNIX User Request TemplateDocumento3 páginasUAM UNIX User Request Templatevamsee_mkAinda não há avaliações
- RUFFA MAE CAGALINGAN - Computer Access Request FormDocumento118 páginasRUFFA MAE CAGALINGAN - Computer Access Request FormRenzoGarciaAinda não há avaliações
- Applications Access Request Form Template IndoaksaraDocumento1 páginaApplications Access Request Form Template Indoaksaraimat rohimatAinda não há avaliações
- CDOT Access Request Form - Extender 07172014Documento3 páginasCDOT Access Request Form - Extender 07172014Chrome PicassoAinda não há avaliações
- Access Form To Obama CareDocumento3 páginasAccess Form To Obama CareHarry the GreekAinda não há avaliações
- Joining Kit - TEILDocumento2 páginasJoining Kit - TEILShivam SarohaAinda não há avaliações
- Intranet, Internet and Email Access It Service DeskDocumento1 páginaIntranet, Internet and Email Access It Service DeskJasper Kenneth PeraltaAinda não há avaliações
- PF012.3 Application and Induction PackDocumento14 páginasPF012.3 Application and Induction PackJide SeyiAinda não há avaliações
- Examination Registration Form: Business ConfidentialDocumento22 páginasExamination Registration Form: Business ConfidentialPabloAinda não há avaliações
- Fellow Application Form - SFLBDocumento2 páginasFellow Application Form - SFLBnicehornetAinda não há avaliações
- HTC2022061301 R4 Maintenance Link MetroE 248006-248001Documento13 páginasHTC2022061301 R4 Maintenance Link MetroE 248006-248001LêAnhĐứcAinda não há avaliações
- PMP Application FormDocumento13 páginasPMP Application Formhread76100% (1)
- Instructions CandidatesDocumento10 páginasInstructions CandidatesNaman SahaiAinda não há avaliações
- Exam Reg FormDocumento22 páginasExam Reg Formmaddy1020Ainda não há avaliações
- NHO (1) - EDITED - Insert Watermark - Insert WatermarkDocumento19 páginasNHO (1) - EDITED - Insert Watermark - Insert Watermarkdhivyaaa3011Ainda não há avaliações
- TGEMS Service Request Form (Ver 5.9)Documento1 páginaTGEMS Service Request Form (Ver 5.9)Guti Vicente FernandezAinda não há avaliações
- GOI DoT Acct XferDocumento2 páginasGOI DoT Acct Xferabc_dAinda não há avaliações
- As/400 Sungard: CMSD - Computer Security Authorization/Change Request Form (Csa/Cr)Documento2 páginasAs/400 Sungard: CMSD - Computer Security Authorization/Change Request Form (Csa/Cr)Laura ParkaAinda não há avaliações
- PNP Request FormDocumento1 páginaPNP Request FormatilabayatAinda não há avaliações
- Final Runbook IPT-AmolDocumento119 páginasFinal Runbook IPT-AmolganeshAinda não há avaliações
- 2.3 PMI SP Certification ApplicationDocumento10 páginas2.3 PMI SP Certification Applicationᗩᒫᕦ᙭ ᙜᙜᘜAinda não há avaliações
- Ad Hoc Report Request: ASE Estern Eserve NiversityDocumento3 páginasAd Hoc Report Request: ASE Estern Eserve NiversityJafarAinda não há avaliações
- 02.borang User RegistrationDocumento2 páginas02.borang User Registrationsuhairizwan ab wahabAinda não há avaliações
- Joining Kit - 2021 - Version 2Documento4 páginasJoining Kit - 2021 - Version 2cocacola_thandaAinda não há avaliações
- GWHS Web Hosting - H002Documento6 páginasGWHS Web Hosting - H002Jeshian YradAinda não há avaliações
- Sample Document - Joining Kit For EPDocumento5 páginasSample Document - Joining Kit For EPkish100% (1)
- Revised Diploma FormDocumento5 páginasRevised Diploma FormNivedan kumarAinda não há avaliações
- User Story ExampleDocumento3 páginasUser Story ExampleKamya JangAinda não há avaliações
- Privileged User ApplDocumento2 páginasPrivileged User ApplSpit FireAinda não há avaliações
- Bhavishya DDODocumento25 páginasBhavishya DDORamanathan Srinivasan50% (2)
- From: Date: To: Head - Human ResourcesDocumento4 páginasFrom: Date: To: Head - Human Resourcesgehnau100% (1)
- Using The Configuration Item (CI) Import TemplateDocumento2 páginasUsing The Configuration Item (CI) Import TemplateQC SriprasitAinda não há avaliações
- Acc111 Register VendorDocumento3 páginasAcc111 Register Vendornandi productsAinda não há avaliações
- 1 - Data Governance Pres - Data ProtectionDocumento23 páginas1 - Data Governance Pres - Data Protectionhlipicenishopping-sophieAinda não há avaliações
- Remote Access Request FormDocumento6 páginasRemote Access Request FormShailesh ShekharAinda não há avaliações
- Applicable For New Application and Plan RenewalDocumento1 páginaApplicable For New Application and Plan RenewalMaraAinda não há avaliações
- LecturingDocumento7 páginasLecturinghutchinson692000Ainda não há avaliações
- Eclaims ManualDocumento32 páginasEclaims ManualnaharmampillyAinda não há avaliações
- SC Forms ComputerAccountRequestDocumento3 páginasSC Forms ComputerAccountRequestMustafa JumaAinda não há avaliações
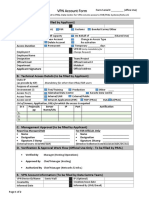
- VPN Account Form: Applicant SignatureDocumento2 páginasVPN Account Form: Applicant SignatureMarium MuhammadAinda não há avaliações
- 2 User Support Form PPADBDocumento1 página2 User Support Form PPADBBonolo SetumeAinda não há avaliações
- No Due Clearance FormDocumento2 páginasNo Due Clearance FormCAE CoreelAinda não há avaliações
- ESS CircularDocumento5 páginasESS CircularramaforuAinda não há avaliações
- I Would Like To Apply For Accreditation As:: AF-PCN-A1Documento3 páginasI Would Like To Apply For Accreditation As:: AF-PCN-A1ThE EyE KaRmAAinda não há avaliações
- Application FormDocumento3 páginasApplication FormHudaAinda não há avaliações
- Employee Casual Leave Form: Dept. Cs&E Skit 2019-20Documento5 páginasEmployee Casual Leave Form: Dept. Cs&E Skit 2019-20DivyaAinda não há avaliações
- ED CV Hi JoDocumento2 páginasED CV Hi JoOmar RoudAinda não há avaliações
- Initial NOP ApplicationDocumento4 páginasInitial NOP ApplicationTamil SelviAinda não há avaliações
- Form RGM Graduate Membership Renew 20190604Documento3 páginasForm RGM Graduate Membership Renew 20190604ahmedanyAinda não há avaliações
- BIT TBI Application NewDocumento6 páginasBIT TBI Application Newteja4u007Ainda não há avaliações
- Background Check Form: Mobile NoDocumento3 páginasBackground Check Form: Mobile NoAbhishek JadhavAinda não há avaliações
- NIFT Digital CertificatesDocumento6 páginasNIFT Digital CertificatesNaval VaswaniAinda não há avaliações
- Requirement PDFDocumento3 páginasRequirement PDFM AbdullahAinda não há avaliações
- Step by Step Guide To Create EIT in Oracle HRMSDocumento37 páginasStep by Step Guide To Create EIT in Oracle HRMSMaged Ali100% (1)
- IT Help Desk TutorialDocumento6 páginasIT Help Desk TutorialHermawan SuheriAinda não há avaliações
- NSR Annexure PDFDocumento6 páginasNSR Annexure PDFSatyanarayan MahantaAinda não há avaliações
- DH E-FormDocumento4 páginasDH E-FormsbspuAinda não há avaliações
- 9713 Applied Ict: MARK SCHEME For The May/June 2010 Question Paper For The Guidance of TeachersDocumento8 páginas9713 Applied Ict: MARK SCHEME For The May/June 2010 Question Paper For The Guidance of TeachersAhmed ZiadAinda não há avaliações
- Access Manual - How To Get Started 2022Documento14 páginasAccess Manual - How To Get Started 2022Rahul Kumar MishraAinda não há avaliações
- POCSO Act - Providing Child-Friendly Judicial Process: TH THDocumento7 páginasPOCSO Act - Providing Child-Friendly Judicial Process: TH THnavalgajjarAinda não há avaliações
- Succession (Final)Documento14 páginasSuccession (Final)dodong123100% (1)
- 4.a.b. Ruby - v. - Espejo PDFDocumento9 páginas4.a.b. Ruby - v. - Espejo PDFervingabralagbonAinda não há avaliações
- Bug Game Dot To Dot Counting 2018Documento1 páginaBug Game Dot To Dot Counting 2018sneAinda não há avaliações
- Dayawon, YoingcoDocumento15 páginasDayawon, YoingcoRaihan Vincent CardenasAinda não há avaliações
- Bussiness Law Exam 2Documento4 páginasBussiness Law Exam 2Morely MejiaAinda não há avaliações
- Rosario Astudillo Vs PP GR No 159734Documento1 páginaRosario Astudillo Vs PP GR No 159734Roosevelt GuerreroAinda não há avaliações
- Executive Order Number 9, PlebDocumento3 páginasExecutive Order Number 9, PlebEarl Russell S Paulican100% (1)
- Sections List:-Business Law: Ca Ankit OberoiDocumento8 páginasSections List:-Business Law: Ca Ankit OberoiAkash BabuAinda não há avaliações
- EQUATORIAL V Sps DesiderioDocumento7 páginasEQUATORIAL V Sps DesiderioRogie ToriagaAinda não há avaliações
- Lang Naman Ang Gagawin Niyan, Right?Documento2 páginasLang Naman Ang Gagawin Niyan, Right?mjpjoreAinda não há avaliações
- Crimpro Third SetDocumento32 páginasCrimpro Third Setnicole hinanayAinda não há avaliações
- People v. Ivler y AguilarDocumento2 páginasPeople v. Ivler y AguilarcenAinda não há avaliações
- Notes On Intellectual Property (Ip) Law: Mylene I. Amerol - MacumbalDocumento41 páginasNotes On Intellectual Property (Ip) Law: Mylene I. Amerol - MacumbalAlain BarbaAinda não há avaliações
- Dinakaran 4th RepresentationDocumento11 páginasDinakaran 4th RepresentationJudicialReformsAinda não há avaliações
- CIR vs. Isabela Cultural Corp., G.R. No. 172231Documento3 páginasCIR vs. Isabela Cultural Corp., G.R. No. 172231Ronz RoganAinda não há avaliações
- Halili V CIR DigestDocumento1 páginaHalili V CIR Digestronhuman14100% (2)
- Tijam V Sibonghanoy. L-21450. Apr 15 1968Documento1 páginaTijam V Sibonghanoy. L-21450. Apr 15 1968Raymond Adrian Padilla ParanAinda não há avaliações
- Nacague v. Sulpicio Lines GR 172589, August 8, 2010Documento2 páginasNacague v. Sulpicio Lines GR 172589, August 8, 2010Bion Henrik PrioloAinda não há avaliações
- Salonga vs. Warner Barnes and Co.Documento4 páginasSalonga vs. Warner Barnes and Co.Teoti Navarro ReyesAinda não há avaliações
- Doctrine of Public AccountabilityDocumento6 páginasDoctrine of Public AccountabilityAmanDasAinda não há avaliações
- Middleeast Chamber SummonsDocumento2 páginasMiddleeast Chamber SummonsfedwredAinda não há avaliações
- Macayan - Cabiguez CaseDocumento45 páginasMacayan - Cabiguez CaseJesimiel CarlosAinda não há avaliações
- SecretaryDocumento41 páginasSecretaryLim Yew TongAinda não há avaliações
- People V PincalinDocumento2 páginasPeople V PincalinMikhel BeltranAinda não há avaliações
- Final Examinations Political LawDocumento8 páginasFinal Examinations Political LawFelice Juleanne Lador-EscalanteAinda não há avaliações
- Re: 2003 BAR EXAMINATIONSDocumento23 páginasRe: 2003 BAR EXAMINATIONSJosephine BercesAinda não há avaliações
- The Punjab Office of The Ombudsman Act 1997Documento10 páginasThe Punjab Office of The Ombudsman Act 1997Salman Ur RashidAinda não há avaliações
- Espinas Vs CoaDocumento3 páginasEspinas Vs Coachatmche-06Ainda não há avaliações
- AlcDocumento2 páginasAlcAshish RaiAinda não há avaliações