Você também pode gostar
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Meniere's Disease.Documento30 páginasMeniere's Disease.June Yasa HacheroAinda não há avaliações
- Ménière's Disease: Drop AttacksDocumento4 páginasMénière's Disease: Drop AttacksFenita Renny DinataAinda não há avaliações
- Meniere's Disease: What Is Ménières Disease?Documento4 páginasMeniere's Disease: What Is Ménières Disease?Deborah Bravian TairasAinda não há avaliações
- Mineire'sDocumento16 páginasMineire'sShaykh Evangelista BacualAinda não há avaliações
- RN Pharmacology IV Push ReferanceDocumento12 páginasRN Pharmacology IV Push ReferanceMissK2216Ainda não há avaliações
- PIN2215 Trigger Point InjectionsDocumento3 páginasPIN2215 Trigger Point InjectionsBob AdleAinda não há avaliações
- Otosclerosis and Menieres DiseaseDocumento5 páginasOtosclerosis and Menieres DiseaseYoko Mae YanoAinda não há avaliações
- Neurogenic Shock (New)Documento14 páginasNeurogenic Shock (New)Syarafina AminuddinAinda não há avaliações
- 10 1097@01 JAA 0000522145 52305 AaDocumento2 páginas10 1097@01 JAA 0000522145 52305 AaAwal Safar M100% (1)
- STDDocumento78 páginasSTDKrupa KarnikAinda não há avaliações
- Infection Control Committee 6 Icc. Meeting DATE: MAY 22, 2020 TIME: 11:50 AM - 3:40 PM Venue: Board Room, Administrative Office 10Th FloorDocumento7 páginasInfection Control Committee 6 Icc. Meeting DATE: MAY 22, 2020 TIME: 11:50 AM - 3:40 PM Venue: Board Room, Administrative Office 10Th FloorCris GalendezAinda não há avaliações
- Understanding Traumatic Brain InjuryDocumento43 páginasUnderstanding Traumatic Brain InjurySilvanaPutriAinda não há avaliações
- IV Push List PedsDocumento5 páginasIV Push List PedskrizzywhizzyAinda não há avaliações
- Burns: Major and Minor BurnsDocumento25 páginasBurns: Major and Minor BurnsTrisha TannerAinda não há avaliações
- Muscle Strength TestingDocumento3 páginasMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
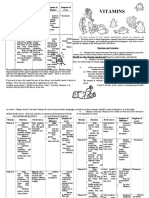
- Vitamin Function Food Sources Symptom of Deficiency Symptom of ExcessDocumento3 páginasVitamin Function Food Sources Symptom of Deficiency Symptom of ExcessBimo OmibAinda não há avaliações
- Tetanus RabiesDocumento67 páginasTetanus RabiesWaNda GrAinda não há avaliações
- Telehealth Physical Exam: Eyes Neck Chest SkinDocumento1 páginaTelehealth Physical Exam: Eyes Neck Chest SkinYazeed QadadhaAinda não há avaliações
- Meniere DiseaseDocumento16 páginasMeniere DiseaseNavjot Brar100% (2)
- Eming Report Precipitous LaborDocumento11 páginasEming Report Precipitous LaborJudeLaxAinda não há avaliações
- Urinary SystemDocumento10 páginasUrinary SystemElyka Alivan Valdez PolonioAinda não há avaliações
- Burns Pathophysiology 2Documento1 páginaBurns Pathophysiology 2Monique Ann DanoyAinda não há avaliações
- Check ListDocumento11 páginasCheck ListtetarwalAinda não há avaliações
- Chapter 14 Intravenous Solutions, Equipment, and CalculationsDocumento48 páginasChapter 14 Intravenous Solutions, Equipment, and CalculationsEn Ras100% (1)
- Nursing Care Plan: Ineffective CopingDocumento2 páginasNursing Care Plan: Ineffective CopingRosalinda SalvadorAinda não há avaliações
- Migraine LeafletDocumento6 páginasMigraine LeafletEliza SitinjakAinda não há avaliações
- ConjunctivitisDocumento18 páginasConjunctivitisPrashanth Padmini VenugopalAinda não há avaliações
- Head Trauma: Adhitya Rahadi, M.DDocumento50 páginasHead Trauma: Adhitya Rahadi, M.DNatasya Saraswati100% (1)
- Suctioning: Prepared By: Christian Ravina M.sc. (N), 2 Year M.T.I.N. ChangaDocumento25 páginasSuctioning: Prepared By: Christian Ravina M.sc. (N), 2 Year M.T.I.N. ChangaGrace GurdielAinda não há avaliações
- Case Report Chronic TonsilitisDocumento12 páginasCase Report Chronic TonsilitisKarunia Dias BhaskoroAinda não há avaliações
- Pain and Pain ManagementDocumento7 páginasPain and Pain ManagementNatukunda DianahAinda não há avaliações
- Brain TumorDocumento50 páginasBrain TumorbudiAinda não há avaliações
- Jarvis 12 Skin Hair NailsDocumento11 páginasJarvis 12 Skin Hair NailsSarah C. SnooksAinda não há avaliações
- TBI Understanding TBI Part 1Documento4 páginasTBI Understanding TBI Part 1LindseyRae ParkerAinda não há avaliações
- Homeostasis Temperature RegulationDocumento22 páginasHomeostasis Temperature RegulationChris AllamAinda não há avaliações
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocumento6 páginasChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersAinda não há avaliações
- Penile CancerDocumento18 páginasPenile CancerSmiley QueenAinda não há avaliações
- How Does Radiation Therapy Work?Documento5 páginasHow Does Radiation Therapy Work?mikeadrianAinda não há avaliações
- Graves DseDocumento5 páginasGraves DseHester Marie SimpiaAinda não há avaliações
- InhalDocumento33 páginasInhallupeAinda não há avaliações
- LaryngitisDocumento9 páginasLaryngitisjonna casumpangAinda não há avaliações
- Bowel Obstruction SurgeryDocumento12 páginasBowel Obstruction SurgeryDivya JoyAinda não há avaliações
- Random Blood Sugar Estimation and Its SignificanceDocumento11 páginasRandom Blood Sugar Estimation and Its Significanceapi-38237850% (1)
- Wound Dressings Update: Carolina Weller, Geoff SussmanDocumento7 páginasWound Dressings Update: Carolina Weller, Geoff SussmanyodinheimAinda não há avaliações
- UTI (Urinary Tract Infection)Documento9 páginasUTI (Urinary Tract Infection)Carson BirthAinda não há avaliações
- DR TahirDocumento61 páginasDR TahirRohail GulAinda não há avaliações
- Cognitive DisorderDocumento72 páginasCognitive DisorderJamal P. AlawiyaAinda não há avaliações
- Alternative & Complementary Therapies: Play Therapy, Group/Individual Therapy, Yoga, ExerciseDocumento32 páginasAlternative & Complementary Therapies: Play Therapy, Group/Individual Therapy, Yoga, ExerciseVanetAinda não há avaliações
- TetanusDocumento3 páginasTetanusRoma Nova Pascual CabarrubiasAinda não há avaliações
- Basic Laparotomy InstrumentsDocumento10 páginasBasic Laparotomy InstrumentsJordan Cruz100% (1)
- How To Define CardiomegalyDocumento2 páginasHow To Define CardiomegalyKjean De Vera MelendezAinda não há avaliações
- mhGAP Humanitarian Intervention Guide (mhGAP-HIG) - English VersionDocumento68 páginasmhGAP Humanitarian Intervention Guide (mhGAP-HIG) - English VersionПламен МинчевAinda não há avaliações
- Ely. Delirium SlidesDocumento51 páginasEly. Delirium SlidesParvathy R NairAinda não há avaliações
- Assessment Renal CalculiDocumento2 páginasAssessment Renal CalculiLeslie LuscombeAinda não há avaliações
- Asthma: A. DefinitionDocumento6 páginasAsthma: A. DefinitionElvando SimatupangAinda não há avaliações
- Open and Closed FractureDocumento22 páginasOpen and Closed FractureHesanRajaraniAinda não há avaliações
- Retinal DetachmentDocumento8 páginasRetinal DetachmentMaisarah BakariAinda não há avaliações
- Asthma: Prepared by Fatima Hirzallah RN, MSN, CNS, PHDDocumento21 páginasAsthma: Prepared by Fatima Hirzallah RN, MSN, CNS, PHDناصر دويكاتAinda não há avaliações
- POTANGINADocumento18 páginasPOTANGINAJames DapatAinda não há avaliações
- Existentialism, Phenomenology and EducationDocumento43 páginasExistentialism, Phenomenology and Educationrosminiaisyah0% (1)
- Service Innovation and DesignDocumento23 páginasService Innovation and DesignMahfuzur Rahman100% (1)
- Mkane Ngss Lesson Planning TemplateDocumento2 páginasMkane Ngss Lesson Planning Templateapi-85725330Ainda não há avaliações
- ACT-Fundamentos ConceptualesDocumento34 páginasACT-Fundamentos ConceptualesLeo Edison C JAinda não há avaliações
- Assignment Curricullum EvaluationDocumento12 páginasAssignment Curricullum EvaluationushaAinda não há avaliações
- Acc Behaviour 1Documento34 páginasAcc Behaviour 1nabilAinda não há avaliações
- Module 7 Artistic and Creativity LiteracyDocumento6 páginasModule 7 Artistic and Creativity LiteracyElla Marie DeñolaAinda não há avaliações
- Consuelo Gallegos-Ayala 2 1Documento3 páginasConsuelo Gallegos-Ayala 2 1api-519799744Ainda não há avaliações
- Final Humanities DanceDocumento30 páginasFinal Humanities DanceSally JabelAinda não há avaliações
- TarzanDocumento25 páginasTarzanMonish BossAinda não há avaliações
- Icf Core Competencies Rating LevelsDocumento11 páginasIcf Core Competencies Rating LevelsAdityaImannudinSuryomurtjitoAinda não há avaliações
- Chapter 4 AssessmentDocumento46 páginasChapter 4 AssessmentKarla Kim Yanguas GragasinAinda não há avaliações
- The Kinslow System Your Path To Proven Success in Health Love and Life PDFDocumento20 páginasThe Kinslow System Your Path To Proven Success in Health Love and Life PDFAmy Louise Platt Ferreira0% (5)
- Organisational Change PDFDocumento107 páginasOrganisational Change PDFMo XiuRenAinda não há avaliações
- Worksheet (1) Lailatul Maghfirah 2161201105Documento4 páginasWorksheet (1) Lailatul Maghfirah 2161201105Lailatul MaghfirahAinda não há avaliações
- Disha Quick Revision English Core MindMaps C 12 @crackjee XyzDocumento32 páginasDisha Quick Revision English Core MindMaps C 12 @crackjee XyzSubhrajyoti BanerjeeAinda não há avaliações
- Belbin Team Roles QuestionnaireDocumento3 páginasBelbin Team Roles Questionnaireapi-248119294Ainda não há avaliações
- Different Graphic OrganizerDocumento46 páginasDifferent Graphic OrganizerJEZZA MEH MAGHAMILAinda não há avaliações
- Exam Marking RubricDocumento1 páginaExam Marking RubricasdjalsdkAinda não há avaliações
- Test Bank For Organizational Behavior Science The Real World and You 8th Edition by NelsonDocumento36 páginasTest Bank For Organizational Behavior Science The Real World and You 8th Edition by Nelsontoadletgeand1j4d100% (42)
- Do You Think Bullying Is A Serious Issue in Your SchoolDocumento7 páginasDo You Think Bullying Is A Serious Issue in Your Schoolawrikah alphardliebe100% (2)
- A Comparative Study of Alienation Among Urban and Rural College Students of Delhi UniversityDocumento5 páginasA Comparative Study of Alienation Among Urban and Rural College Students of Delhi UniversityInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Sol3e Preint U0 Short Test 1bDocumento1 páginaSol3e Preint U0 Short Test 1bГалина Яковлева100% (2)
- John Watson and Burrhus Frederick SkinnerDocumento16 páginasJohn Watson and Burrhus Frederick SkinnerMerkelly DelesAinda não há avaliações
- The Benefits of Laughter On Mental Health - Persuasive EssayDocumento3 páginasThe Benefits of Laughter On Mental Health - Persuasive EssayNoura AttiaAinda não há avaliações
- Performance and Affects: From Eros To ThanathosDocumento41 páginasPerformance and Affects: From Eros To ThanathosCozmolici BiatriceAinda não há avaliações
- The Impact of Brand Prestige On Trust Perceived Risk Satisfaction and Loyalty in Upscale RestaurantsDocumento25 páginasThe Impact of Brand Prestige On Trust Perceived Risk Satisfaction and Loyalty in Upscale RestaurantsM SalAinda não há avaliações
- PR 1Documento26 páginasPR 1Giah Morales ValenciaAinda não há avaliações
- Roject Eport: Ubmitted in Artial Fulfilment of The Requirements of Program OF Chool F Anagement Niversity UrgaonDocumento38 páginasRoject Eport: Ubmitted in Artial Fulfilment of The Requirements of Program OF Chool F Anagement Niversity UrgaonGaurav ChhabraAinda não há avaliações