Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Anti Epileptic Drugs Effect On GrowthDocumento17 páginasAnti Epileptic Drugs Effect On Growthtom24Ainda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Nej Mo A 1610020Documento14 páginasNej Mo A 1610020Nurul Khairiyah AmriAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Nej Mo A 1412082Documento11 páginasNej Mo A 1412082tom24Ainda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Nej Mo A 1503093Documento12 páginasNej Mo A 1503093tom24Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Weight Gain and Height Growth During Infancy, Childhood, and Adolescence As Predictors of Adult Cardiovascular RiskDocumento12 páginasWeight Gain and Height Growth During Infancy, Childhood, and Adolescence As Predictors of Adult Cardiovascular Risktom24Ainda não há avaliações
- Cover Jurnal ReadingDocumento1 páginaCover Jurnal Readingtom24Ainda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Nej Mo A 1314768Documento10 páginasNej Mo A 1314768tom24Ainda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
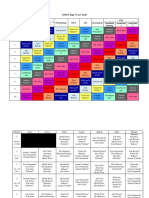
- Jadwal Jaga Co Ass AnakDocumento5 páginasJadwal Jaga Co Ass Anaktom24Ainda não há avaliações
- 2010 Rapid Review of Radiology (2010) (True PDF) (4.5-Star) PDFDocumento353 páginas2010 Rapid Review of Radiology (2010) (True PDF) (4.5-Star) PDFtom24100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Dr. Rosi - CPAPDocumento65 páginasDr. Rosi - CPAPtom24Ainda não há avaliações
- Congenital and Acquired Bone Marrow Failure: 1st EditionDocumento9 páginasCongenital and Acquired Bone Marrow Failure: 1st EditiontotoirsyadAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Kementerian Kesehatan Republik Indonesia Jilid 2Documento1 páginaKementerian Kesehatan Republik Indonesia Jilid 2tom24Ainda não há avaliações
- Dr. Sudung - Tata Laksana Krisis HipertensiDocumento30 páginasDr. Sudung - Tata Laksana Krisis Hipertensitom24Ainda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Jurnal FixDocumento12 páginasJurnal FixYogi Ardhi IrafaniAinda não há avaliações
- Weight-For-Height BOYS: 2 To 5 Years (Z-Scores)Documento1 páginaWeight-For-Height BOYS: 2 To 5 Years (Z-Scores)Malisa Lukman100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Stase Anak Periode 28 NovemberDocumento2 páginasStase Anak Periode 28 Novembertom24Ainda não há avaliações
- Modul 2Documento54 páginasModul 2tom24Ainda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Modul 1Documento40 páginasModul 1tom24Ainda não há avaliações
- Httpsjkbopee Gov InPdfDownloader Ashxnid 13580&type NDocumento221 páginasHttpsjkbopee Gov InPdfDownloader Ashxnid 13580&type NMONISAinda não há avaliações
- Senile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyDocumento6 páginasSenile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyadliahghaisaniAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- NHP Original 1985 PDFDocumento4 páginasNHP Original 1985 PDFAndrei IordanAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Caravan Tourism in West BengalDocumento2 páginasCaravan Tourism in West BengalUddipan NathAinda não há avaliações
- Your Electricity BillDocumento8 páginasYour Electricity BillE EeAinda não há avaliações
- Sudeep SrivastavaDocumento202 páginasSudeep Srivastavasandeepsrivastava41Ainda não há avaliações
- TOPHEALTH SUNOF+ Ethylhexyl-P-Methoxycinnamate, 2-Ethylhexy MsdsDocumento7 páginasTOPHEALTH SUNOF+ Ethylhexyl-P-Methoxycinnamate, 2-Ethylhexy MsdsTOP HEALTH ALRROMIAinda não há avaliações
- NFPA Codes & Standards - 10Documento1 páginaNFPA Codes & Standards - 10karpanaiAinda não há avaliações
- Mental Practice in Chronic StrokeDocumento6 páginasMental Practice in Chronic StrokeIsa AbdantauhidAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Dupuytren's ContractureDocumento273 páginasDupuytren's Contractureslaughteringtheposer100% (1)
- Reimplantation of Avulsed Tooth - A Case StudyDocumento3 páginasReimplantation of Avulsed Tooth - A Case Studyrahul sharmaAinda não há avaliações
- Nqs NQSDocumento270 páginasNqs NQSManpreet KaurAinda não há avaliações
- Periodontal Probing and Techniques JCDocumento58 páginasPeriodontal Probing and Techniques JCAbhay TandonAinda não há avaliações
- The Trade Effluents (Prescribed Processes and Substances) Regulations 1992Documento2 páginasThe Trade Effluents (Prescribed Processes and Substances) Regulations 1992Lúcio FernandesAinda não há avaliações
- A Portfolio For Work Immersion Business Enterprise SimulationDocumento17 páginasA Portfolio For Work Immersion Business Enterprise SimulationnicAinda não há avaliações
- Useful BooksDocumento3 páginasUseful BooksphuongfeoAinda não há avaliações
- Perdev Week 5Documento3 páginasPerdev Week 5AdiraAinda não há avaliações
- Errors of Eye Refraction and HomoeopathyDocumento11 páginasErrors of Eye Refraction and HomoeopathyDr. Rajneesh Kumar Sharma MD HomAinda não há avaliações
- Garrison, NancyDocumento139 páginasGarrison, NancyBrunoAinda não há avaliações
- Reszon Pi - Typhidot Rapid Igm 2011-01Documento2 páginasReszon Pi - Typhidot Rapid Igm 2011-01Harnadi WonogiriAinda não há avaliações
- CapsicumDocumento32 páginasCapsicumpk_shahanaAinda não há avaliações
- Practical Research 2Documento6 páginasPractical Research 2meioAinda não há avaliações
- 2014 Academic Calendar Semester 1Documento1 página2014 Academic Calendar Semester 1RuqqqAinda não há avaliações
- Midwives and Nutrition Education During Pregnancy - A Literature RDocumento23 páginasMidwives and Nutrition Education During Pregnancy - A Literature RSuredaAinda não há avaliações
- Beast ModeDocumento5 páginasBeast ModeMizulIkhsanMazlan100% (1)
- Bài tập tiếng anhDocumento8 páginasBài tập tiếng anhLinh KhánhAinda não há avaliações
- David Carreras - A Cunnilinguist's Guide To Mind-Blowing Oral SexDocumento6 páginasDavid Carreras - A Cunnilinguist's Guide To Mind-Blowing Oral SexKostyaAinda não há avaliações
- Time Management StrategiesDocumento3 páginasTime Management Strategiesأحمد عبدالمحسنAinda não há avaliações
- State School Immunization Requirements and Vaccine Exemption LawsDocumento18 páginasState School Immunization Requirements and Vaccine Exemption LawsBen CulpepperAinda não há avaliações
- American Architecture Began With Frank Lloyd WrightDocumento8 páginasAmerican Architecture Began With Frank Lloyd WrightAdheith South NgalamAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)