Você também pode gostar
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderAinda não há avaliações
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyNo EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyNota: 1 de 5 estrelas1/5 (1)
- Effects of Diet and Simvastatin On Serum Lipids, Insulin, and Antioxidants in Hypercholesterolemic MenDocumento8 páginasEffects of Diet and Simvastatin On Serum Lipids, Insulin, and Antioxidants in Hypercholesterolemic MenAranel BomAinda não há avaliações
- CometDocumento9 páginasCometSohail AhmedAinda não há avaliações
- Stellar CrestorDocumento9 páginasStellar CrestorMarwan NasriAinda não há avaliações
- Lyon Diet Heart Study - de Lorgeril 1994Documento6 páginasLyon Diet Heart Study - de Lorgeril 1994acolpoAinda não há avaliações
- SerumDocumento6 páginasSerumdindaAinda não há avaliações
- Effects of Omega-3 Supplementation On Serum Triglyceride Levels in Adults With Hypertriglyceridemia: A Systematic ReviewDocumento21 páginasEffects of Omega-3 Supplementation On Serum Triglyceride Levels in Adults With Hypertriglyceridemia: A Systematic Reviewapi-513839411Ainda não há avaliações
- Nej Mo A 1411487Documento10 páginasNej Mo A 1411487Liana PuspitasariAinda não há avaliações
- CLC 4960230910Documento7 páginasCLC 4960230910walnut21Ainda não há avaliações
- DMJ 37 465Documento10 páginasDMJ 37 465sn4s7nyxcbAinda não há avaliações
- Cardiovascular PacketDocumento23 páginasCardiovascular Packetapi-573199099Ainda não há avaliações
- Paper Title: (16 Bold)Documento9 páginasPaper Title: (16 Bold)vegeto portmanAinda não há avaliações
- Tousoulis 2005 NODocumento4 páginasTousoulis 2005 NONismalaAinda não há avaliações
- Outcomes of Obese, Clozapine-Treated Inpatients With Schizophrenia Placed On A Six-Month Diet and Physical Activity ProgramDocumento7 páginasOutcomes of Obese, Clozapine-Treated Inpatients With Schizophrenia Placed On A Six-Month Diet and Physical Activity ProgramnajibrendraAinda não há avaliações
- Efficacy and Safety of Monascus Purpureus Went Rice in Subjects With HyperlipidemiaDocumento8 páginasEfficacy and Safety of Monascus Purpureus Went Rice in Subjects With HyperlipidemiaAyshe SlocumAinda não há avaliações
- The Effects of Long-Term Dietary Therapy On Patients With HypertriglyceridemiaDocumento11 páginasThe Effects of Long-Term Dietary Therapy On Patients With Hypertriglyceridemiaraul zea calcinaAinda não há avaliações
- Suplementacao em NutricaoDocumento9 páginasSuplementacao em NutricaoJoyce CamposAinda não há avaliações
- Resting Metabolic Rate of Anorexia Nervosa Patients During Weight GainDocumento10 páginasResting Metabolic Rate of Anorexia Nervosa Patients During Weight GainRyugachi Go SeibaAinda não há avaliações
- Retrospective Case Series of Patients With Diabetes or Prediabetes Who Were Switched From Omega-3-Acid Ethyl Esters To Icosapent EthylDocumento11 páginasRetrospective Case Series of Patients With Diabetes or Prediabetes Who Were Switched From Omega-3-Acid Ethyl Esters To Icosapent EthylAgus SetiawanAinda não há avaliações
- BMC Family PracticeDocumento19 páginasBMC Family PracticeFirda AndiAinda não há avaliações
- Beneficial Effects of Viscous Dietary Fiber From Konjac-Mannan in Subjects With The Insulin Resistance Syndro M eDocumento6 páginasBeneficial Effects of Viscous Dietary Fiber From Konjac-Mannan in Subjects With The Insulin Resistance Syndro M eNaresh MaliAinda não há avaliações
- Nursing Research PresentaionDocumento33 páginasNursing Research Presentaionapi-300699057Ainda não há avaliações
- Efficacy of Autologous Bone Marrow DerivDocumento10 páginasEfficacy of Autologous Bone Marrow DerivsulaymanwaquarAinda não há avaliações
- ID Gambaran Histologik Hati Pada Kelinci Ya PDFDocumento5 páginasID Gambaran Histologik Hati Pada Kelinci Ya PDFYudha Jrokolioli NostAinda não há avaliações
- Omega 3Documento8 páginasOmega 3Mireya AlejandraAinda não há avaliações
- Astaxanthin Improves Glucose Metabolism and Reduces Blood Pressure in Patients With Type 2 Diabetes MellitusDocumento6 páginasAstaxanthin Improves Glucose Metabolism and Reduces Blood Pressure in Patients With Type 2 Diabetes MellitusdaveAinda não há avaliações
- Paper Title: (16 Bold Blue Color)Documento9 páginasPaper Title: (16 Bold Blue Color)Fauzi RusdiantoAinda não há avaliações
- Paper TemplateDocumento10 páginasPaper Templatenur hidayatAinda não há avaliações
- Canola OilDocumento6 páginasCanola OilHilyatulAuliyaBintiHarisAinda não há avaliações
- j3 2010Documento12 páginasj3 2010Taha FransAinda não há avaliações
- A Low-Fat Vegan Diet and A Conventional Diabetes Diet in The Treatment of Type 2 Diabetes: A Randomized, Controlled, 74-wk Clinical TrialDocumento9 páginasA Low-Fat Vegan Diet and A Conventional Diabetes Diet in The Treatment of Type 2 Diabetes: A Randomized, Controlled, 74-wk Clinical TrialSheldon SilvaAinda não há avaliações
- JI X HDL PESQUISA BIBLIOGRAFICADocumento8 páginasJI X HDL PESQUISA BIBLIOGRAFICAJúlia MunizAinda não há avaliações
- The Effect of High-Protein, Low-Carbohydrate Diets in The Treatment of Type 2 Diabetes: A 12 Month Randomised Controlled TrialDocumento10 páginasThe Effect of High-Protein, Low-Carbohydrate Diets in The Treatment of Type 2 Diabetes: A 12 Month Randomised Controlled TrialFirda Rizky KhoerunnissaAinda não há avaliações
- Analysis of Plasm LipoproteinDocumento10 páginasAnalysis of Plasm LipoproteinWilson KhawAinda não há avaliações
- Timmins Lipids 2014 1 Compatibility Mode Lec 4Documento23 páginasTimmins Lipids 2014 1 Compatibility Mode Lec 4parkmparkAinda não há avaliações
- Mussner 2002Documento6 páginasMussner 2002m.viniciusnutriAinda não há avaliações
- BIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherDocumento5 páginasBIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherHisWellnessAinda não há avaliações
- Kidney Paper - 2017Documento9 páginasKidney Paper - 2017samah hossnyAinda não há avaliações
- Ezetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneDocumento9 páginasEzetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneEditor ERWEJAinda não há avaliações
- Anethum Graveolens and Hyperlipidemia: A Randomized Clinical TrialDocumento13 páginasAnethum Graveolens and Hyperlipidemia: A Randomized Clinical TrialYuliantikha Nurul QomariahAinda não há avaliações
- Circulation 1979 Hennekens 486 9Documento5 páginasCirculation 1979 Hennekens 486 9Dwi Putri CAinda não há avaliações
- Panax GinsengDocumento9 páginasPanax GinsengDevi MelissaAinda não há avaliações
- Randomized Controlled Trial of Tinospora Crispa For Additional Therapy in Patients With Type 2 Diabetes MellitusDocumento4 páginasRandomized Controlled Trial of Tinospora Crispa For Additional Therapy in Patients With Type 2 Diabetes MellitusEva SuryantiAinda não há avaliações
- BIOS LIFE - Utah Trial by Dr. Peter J.E. VerdegemDocumento6 páginasBIOS LIFE - Utah Trial by Dr. Peter J.E. VerdegemHisWellnessAinda não há avaliações
- 19 10835Documento7 páginas19 10835LiaaAinda não há avaliações
- Serum Vaspin Concentrations in Human Obesity and Type 2 DiabetesDocumento6 páginasSerum Vaspin Concentrations in Human Obesity and Type 2 DiabetesDianPertiwiSAinda não há avaliações
- Effect of A High-Protein, Low-Carbohydrate Diet On Blood Glucose Control in People With Type 2 DiabetesDocumento8 páginasEffect of A High-Protein, Low-Carbohydrate Diet On Blood Glucose Control in People With Type 2 DiabetesFajar AgAinda não há avaliações
- Perez Pozo2009Documento8 páginasPerez Pozo2009Anonymous 0mtGtB6u3Ainda não há avaliações
- Effects of Probiotic Supplementation On Lipid Profile of Women With Rheumatoid Arthritis: A Randomized Placebo-Controlled Clinical TrialDocumento7 páginasEffects of Probiotic Supplementation On Lipid Profile of Women With Rheumatoid Arthritis: A Randomized Placebo-Controlled Clinical Trialsufiah istthyAinda não há avaliações
- Am J Clin Nutr 2016 Valsesia Ajcn.116.137646Documento10 páginasAm J Clin Nutr 2016 Valsesia Ajcn.116.137646kasabeAinda não há avaliações
- 1 s2.0 S0022316622105067 MainDocumento7 páginas1 s2.0 S0022316622105067 MainqixiadeyouxiangAinda não há avaliações
- Bio 3Documento6 páginasBio 3YISELAAinda não há avaliações
- Turkjmedsci-50-354 PubmedDocumento6 páginasTurkjmedsci-50-354 PubmedRizka Uda'aAinda não há avaliações
- Diabetes MellitusDocumento8 páginasDiabetes Mellitusi_anitaAinda não há avaliações
- Ameliorative Potentialof Thiazolidinedionesand StatinsDocumento6 páginasAmeliorative Potentialof Thiazolidinedionesand StatinsAstrid GanadyaAinda não há avaliações
- Effect of A Late Evening Snack On Outpatients With Liver CirrhosisDocumento7 páginasEffect of A Late Evening Snack On Outpatients With Liver CirrhosisThinh VinhAinda não há avaliações
- Overfeeding TiroideDocumento12 páginasOverfeeding TiroideAimone FerriAinda não há avaliações
- Effects of Omega-3 Fatty Acids On Markers of Inflammation in Patients With Chronic Kidney DiseaseDocumento9 páginasEffects of Omega-3 Fatty Acids On Markers of Inflammation in Patients With Chronic Kidney DiseaseStefanie SuwitaAinda não há avaliações
- 7decaf9c Cb18 4623 Bced Ecef2197e451Documento25 páginas7decaf9c Cb18 4623 Bced Ecef2197e451PrabhuAinda não há avaliações
- Journal Reading MATADocumento9 páginasJournal Reading MATAEvan AlbertAinda não há avaliações
- AGD LatihanDocumento4 páginasAGD LatihanEvan AlbertAinda não há avaliações
- Incident ReportDocumento1 páginaIncident ReportEvan AlbertAinda não há avaliações
- Absensi Morning ReportDocumento1 páginaAbsensi Morning ReportEvan AlbertAinda não há avaliações
- Suture LectureDocumento42 páginasSuture LectureAniz RataniAinda não há avaliações
- Lipasesindairyindustry ReviewDocumento10 páginasLipasesindairyindustry ReviewChinh Đinh ViệtAinda não há avaliações
- Tarif Medical Check Up - Murni Teguh Memorial HospitalDocumento4 páginasTarif Medical Check Up - Murni Teguh Memorial HospitalSR HasibuanAinda não há avaliações
- Classification of Lipids and Their ExamplesDocumento2 páginasClassification of Lipids and Their ExamplesA C100% (1)
- Glycerol BlankingDocumento4 páginasGlycerol BlankingDiah Puspita RiniAinda não há avaliações
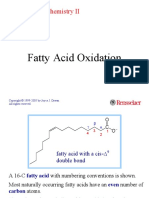
- Fatty Acid Oxidation: Molecular Biochemistry IIDocumento39 páginasFatty Acid Oxidation: Molecular Biochemistry IIDozdi100% (1)
- Nutrition and MetabolismDocumento179 páginasNutrition and Metabolismnursereview100% (9)
- Interrelationship Between Carbohydrate Protein Fat MetabolismDocumento12 páginasInterrelationship Between Carbohydrate Protein Fat MetabolismShailaja Neaupane100% (5)
- Biochem Lec Midterm TransDocumento18 páginasBiochem Lec Midterm TransAndrea Jersey BuluranAinda não há avaliações
- Velocity of Sound in Vegetable OilsDocumento3 páginasVelocity of Sound in Vegetable OilsBramJanssen76Ainda não há avaliações
- Our Objective: What Are Fatty Acids?Documento5 páginasOur Objective: What Are Fatty Acids?Sunita MauryaAinda não há avaliações
- 09 - IB Biology (2016) - 2.3 - Carbohydrates & LipidsDocumento29 páginas09 - IB Biology (2016) - 2.3 - Carbohydrates & LipidsSamuel French RojasAinda não há avaliações
- Edible Oil Brochure (Caracteristicas de Los Catalizadores Pricat)Documento6 páginasEdible Oil Brochure (Caracteristicas de Los Catalizadores Pricat)Victor GaonaAinda não há avaliações
- F08 Healthy Eating and StrokeDocumento20 páginasF08 Healthy Eating and Strokerebreb47Ainda não há avaliações
- Laboratory Manual Practical SBK 3013Documento25 páginasLaboratory Manual Practical SBK 3013SHAFIQAH HANAFIAinda não há avaliações
- Lipids: What Are Fatty Acids?Documento7 páginasLipids: What Are Fatty Acids?Jeff MorrowAinda não há avaliações
- BOOK - FAO (2002) Hal 14-15Documento93 páginasBOOK - FAO (2002) Hal 14-15Zulfadin HanaAinda não há avaliações
- Pauline Lowrie - AQA AS - A Level Year 1 Biology Student Guide - Topics 1 and 2 (2015)Documento97 páginasPauline Lowrie - AQA AS - A Level Year 1 Biology Student Guide - Topics 1 and 2 (2015)Victor TrươngAinda não há avaliações
- Applications of LipaseDocumento14 páginasApplications of LipasetigrenagualAinda não há avaliações
- Copyofmysteryboxquiz Docx 1Documento5 páginasCopyofmysteryboxquiz Docx 1api-319863011Ainda não há avaliações
- Kenny Sap. Value of OilDocumento37 páginasKenny Sap. Value of Oilotaken6Ainda não há avaliações
- Biosynthesis, Characterization and Enzymatic Transesteri Cation of Single Cell Oil of Mucor Circinelloides - A Sustainable Pathway For Biofuel ProductionDocumento7 páginasBiosynthesis, Characterization and Enzymatic Transesteri Cation of Single Cell Oil of Mucor Circinelloides - A Sustainable Pathway For Biofuel Productionveliger100Ainda não há avaliações
- LIPID METABOLISM Notes PDFDocumento8 páginasLIPID METABOLISM Notes PDFToga BrandonAinda não há avaliações
- LayoutDocumento55 páginasLayoutHenok Moges KassahunAinda não há avaliações
- 04 Chapter 1Documento24 páginas04 Chapter 1buddhahandAinda não há avaliações
- 8.1 Biological MoleculesDocumento134 páginas8.1 Biological MoleculesHara Vienna ClivaAinda não há avaliações
- 02042020124642modified - Diet (9 Files Merged)Documento87 páginas02042020124642modified - Diet (9 Files Merged)Stacy ParkerAinda não há avaliações
- 1.2. All Four Biomolecules V2Documento112 páginas1.2. All Four Biomolecules V2Clàudia VicenteAinda não há avaliações
- Biosynthesis of Milk FatDocumento9 páginasBiosynthesis of Milk FatFakhryansyahLuthfianAinda não há avaliações
- Soft Gelatin Capsules (SoftgelsDocumento42 páginasSoft Gelatin Capsules (Softgelsprenatooliveira91% (11)
- Shea ButterDocumento133 páginasShea Buttererica2012Ainda não há avaliações