Você também pode gostar
- Looking Back: Some Reflections on the Prevention and Treatment of Low Back PainNo EverandLooking Back: Some Reflections on the Prevention and Treatment of Low Back PainAinda não há avaliações
- Reflex Control of The Spine and Posture - A Review of The Literature From A Chiropractic PerspectiveDocumento18 páginasReflex Control of The Spine and Posture - A Review of The Literature From A Chiropractic PerspectiveWeeHoe LimAinda não há avaliações
- Rolfing: Reestablishing the Natural Alignment and Structural Integration of the Human Body for Vitality and Well-BeingNo EverandRolfing: Reestablishing the Natural Alignment and Structural Integration of the Human Body for Vitality and Well-BeingNota: 5 de 5 estrelas5/5 (1)
- Exploring Perfect PostureDocumento8 páginasExploring Perfect Posturesquishyware100% (1)
- The Five Diaphragms in Osteopathic Manipulative MeDocumento14 páginasThe Five Diaphragms in Osteopathic Manipulative MeShaun Tyler100% (1)
- Handbook of Us: Understanding and Accepting People with AutismNo EverandHandbook of Us: Understanding and Accepting People with AutismAinda não há avaliações
- SomaticsColorCatalog5 4 06Documento17 páginasSomaticsColorCatalog5 4 06Viviana PueblaAinda não há avaliações
- Trail Guide To The Body: Hand and WristDocumento5 páginasTrail Guide To The Body: Hand and WristBen WisherAinda não há avaliações
- Sensorimotor Training A Global Approach For BalancDocumento9 páginasSensorimotor Training A Global Approach For BalancVizaAinda não há avaliações
- Mindful Motion CaspariDocumento103 páginasMindful Motion CaspariKian Fallahi100% (1)
- Fred L. Mitchell, P. Kai Galen Mitchell - The Muscle Energy Manual Volume Two - Evaluation and Treatment of The Thoracic Spine, Lumbar Spine, and Rib Cage-MET Press (1998)Documento260 páginasFred L. Mitchell, P. Kai Galen Mitchell - The Muscle Energy Manual Volume Two - Evaluation and Treatment of The Thoracic Spine, Lumbar Spine, and Rib Cage-MET Press (1998)Geangu GabrielAinda não há avaliações
- Technique: The Arm LinesDocumento6 páginasTechnique: The Arm LinesEldar SulejmanovicAinda não há avaliações
- Lecture Notes On Psoas & Adductors: Psoas As A Medial RotatorDocumento12 páginasLecture Notes On Psoas & Adductors: Psoas As A Medial RotatorAlisaClark100% (1)
- Physical Therapy Protocols For The Conditions of Hip RegionDocumento50 páginasPhysical Therapy Protocols For The Conditions of Hip RegionAnita GajariAinda não há avaliações
- The Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1Documento9 páginasThe Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1nish0420100% (1)
- Chapmans Reflex 479Documento5 páginasChapmans Reflex 479Huram-abiAinda não há avaliações
- Central Line of Gravity: - Posterior 1/3 of The SkullDocumento9 páginasCentral Line of Gravity: - Posterior 1/3 of The Skullonix2000Ainda não há avaliações
- Diastasis Rectus Abd-InTouch PDFDocumento7 páginasDiastasis Rectus Abd-InTouch PDFIchim AmellyaAinda não há avaliações
- Excerpts From "The Fasciae"Documento24 páginasExcerpts From "The Fasciae"intoilmariAinda não há avaliações
- Radical Unwinding Ebook PDFDocumento76 páginasRadical Unwinding Ebook PDFreetiiiiAinda não há avaliações
- Chapman's Reflexes PointsDocumento10 páginasChapman's Reflexes PointscatalinAinda não há avaliações
- Deep Cervical Fascia by Talha JavedDocumento45 páginasDeep Cervical Fascia by Talha JavedTalha Javed100% (1)
- Neuro Anatomy Nerve TrunksDocumento22 páginasNeuro Anatomy Nerve TrunksDr. Kazuhito Mori100% (1)
- Biomechanics of SpineDocumento9 páginasBiomechanics of SpineAdosotoAinda não há avaliações
- Janda ApproachDocumento5 páginasJanda ApproachMădălina StavaracheAinda não há avaliações
- Visceral Patterns in ScoliDocumento4 páginasVisceral Patterns in ScolileoAinda não há avaliações
- The Helical Ventricular Myocardial Band of Torrent-GuaspDocumento5 páginasThe Helical Ventricular Myocardial Band of Torrent-GuaspTeaKovacevicAinda não há avaliações
- Diri Journal March 2020 Final DiriwebDocumento91 páginasDiri Journal March 2020 Final DiriwebbfbernardesAinda não há avaliações
- Embryology Article John WilksDocumento4 páginasEmbryology Article John Wilkspfi_jenAinda não há avaliações
- Myofascial Meridians As Anatomical Evidence of AcuDocumento9 páginasMyofascial Meridians As Anatomical Evidence of AcuTo MAinda não há avaliações
- The Cervical Spine and Sensorimotor ControlDocumento10 páginasThe Cervical Spine and Sensorimotor Controlpuchio100% (1)
- Diagnostic Touch Its Principles and Application PDFDocumento9 páginasDiagnostic Touch Its Principles and Application PDFJakobStierleAinda não há avaliações
- Structural Integration Origins and DevelopmentDocumento7 páginasStructural Integration Origins and Developmentzac2351Ainda não há avaliações
- Pelvic Stability & Your Core: Written by Diane LeeDocumento9 páginasPelvic Stability & Your Core: Written by Diane LeeisaAinda não há avaliações
- Plasticity FascialDocumento13 páginasPlasticity FascialMichael DuranAinda não há avaliações
- Tom Myers 10 Tips For Fascial Fitness PDFDocumento11 páginasTom Myers 10 Tips For Fascial Fitness PDFslimshader100% (1)
- Female Reproductive System Visceral ManipuationDocumento17 páginasFemale Reproductive System Visceral ManipuationFatemah Beyg100% (1)
- Dermatome MapDocumento12 páginasDermatome MapVivian LiangAinda não há avaliações
- Mechanobiology and Diseases of Mechanotransduction by IngberDocumento14 páginasMechanobiology and Diseases of Mechanotransduction by IngberTensegrity Wiki100% (1)
- Rolf HingesDocumento8 páginasRolf Hingeswalterego58100% (3)
- Working With Appendicular Sciatica, Part III (Myofascial Techniques)Documento5 páginasWorking With Appendicular Sciatica, Part III (Myofascial Techniques)Advanced-Trainings.com100% (3)
- Cranial Rhythmic Impulse Related To The Traube-Hering-Mayer OscillationDocumento11 páginasCranial Rhythmic Impulse Related To The Traube-Hering-Mayer Oscillationthe_walnutAinda não há avaliações
- Diagnostic Touch Parts I IV by Rollin Becker PDFDocumento69 páginasDiagnostic Touch Parts I IV by Rollin Becker PDFCatalin EneAinda não há avaliações
- Muscles of Gait (Biomechanics)Documento25 páginasMuscles of Gait (Biomechanics)Rory CocksAinda não há avaliações
- An Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15Documento24 páginasAn Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15johnAinda não há avaliações
- Lossing BerylArbucklesCranial PDFDocumento67 páginasLossing BerylArbucklesCranial PDFdeemoney3100% (1)
- 2011 Jeremy Lewis Subacromial Impingement SyndromeDocumento11 páginas2011 Jeremy Lewis Subacromial Impingement Syndromepuntocom111Ainda não há avaliações
- Schleip Fascia As A Sensory OrganDocumento28 páginasSchleip Fascia As A Sensory Organignacio camposAinda não há avaliações
- Frozen Shoulder Whitney Lowe Massage MagDocumento4 páginasFrozen Shoulder Whitney Lowe Massage Magwolfgangl70Ainda não há avaliações
- Movement, Stability & Lumbopelvic Pain: Integration of Research and Therapy - Andry VleemingDocumento4 páginasMovement, Stability & Lumbopelvic Pain: Integration of Research and Therapy - Andry VleemingwopegiluAinda não há avaliações
- Temporal Sphenoidal Line T2Documento3 páginasTemporal Sphenoidal Line T2taichi7Ainda não há avaliações
- FeldenkraisDocumento120 páginasFeldenkraiskukutxiAinda não há avaliações
- How A Mysterious Body Part Called Fascia Is Challenging MedicineDocumento16 páginasHow A Mysterious Body Part Called Fascia Is Challenging MedicineWhisperer Bowen100% (1)
- OPP Course Review: John Garlitz, DO Deborah Schmidt, DO Opp 2 April 15, 2015 8:10 AMDocumento248 páginasOPP Course Review: John Garlitz, DO Deborah Schmidt, DO Opp 2 April 15, 2015 8:10 AMmina botross100% (1)
- The Asymmetric Pelvis: Liz Gaggini, M.ADocumento7 páginasThe Asymmetric Pelvis: Liz Gaggini, M.Aleo100% (1)
- Lossing DiagnosingTreatingDu PDFDocumento33 páginasLossing DiagnosingTreatingDu PDFDiana SchlittlerAinda não há avaliações
- The Fascia As Organ of Innerness 2015 EN ChapterDocumento16 páginasThe Fascia As Organ of Innerness 2015 EN ChapterJorge Flores TorresAinda não há avaliações
- Definition and Classification of CPDocumento45 páginasDefinition and Classification of CPMichealowen BabygoalAinda não há avaliações
- Ventilator Management - StatPearls - NCBI BookshelfDocumento13 páginasVentilator Management - StatPearls - NCBI BookshelfHusna LathiifaAinda não há avaliações
- Presentation 4Documento23 páginasPresentation 4Husna LathiifaAinda não há avaliações
- Determinants For Oral Hygiene and Periodontal Status Among Mentally Disabled Children and AdolescentsDocumento7 páginasDeterminants For Oral Hygiene and Periodontal Status Among Mentally Disabled Children and AdolescentsHusna LathiifaAinda não há avaliações
- Pink and White Bordered Floral Friendship Day CardDocumento1 páginaPink and White Bordered Floral Friendship Day CardHusna LathiifaAinda não há avaliações
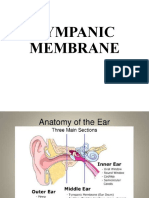
- Tympanic Membrane 1Documento16 páginasTympanic Membrane 1Husna LathiifaAinda não há avaliações
- Logo RshsDocumento1 páginaLogo RshsHusna LathiifaAinda não há avaliações
- Effects of Foot Orthoses With Medial Arch Support and Lateral Wedge On Knee Adduction Moment in Patients With Medial Knee OsteoarthritisDocumento8 páginasEffects of Foot Orthoses With Medial Arch Support and Lateral Wedge On Knee Adduction Moment in Patients With Medial Knee OsteoarthritisHusna LathiifaAinda não há avaliações
- Sarcopenic Dysphagia. A Narrative ReviewDocumento7 páginasSarcopenic Dysphagia. A Narrative ReviewHusna LathiifaAinda não há avaliações
- Core Strength Training For Patients With Chronic Low Back PainDocumento4 páginasCore Strength Training For Patients With Chronic Low Back PainHusna LathiifaAinda não há avaliações
- Mirzaei2018 PDFDocumento7 páginasMirzaei2018 PDFHusna LathiifaAinda não há avaliações
- Functional Performance Testing in Athletes With Functional Ankle InstabilityDocumento10 páginasFunctional Performance Testing in Athletes With Functional Ankle InstabilityHusna LathiifaAinda não há avaliações
- Toorthj 6 544 PDFDocumento4 páginasToorthj 6 544 PDFHusna LathiifaAinda não há avaliações
- Mortality Rate of Patients With Tuberculosis-Destroyed Lung Who Underwent Pulmonary Resection Evidence Based Case ReportDocumento7 páginasMortality Rate of Patients With Tuberculosis-Destroyed Lung Who Underwent Pulmonary Resection Evidence Based Case Reportatls jakartaAinda não há avaliações
- Chapter 4B - Upper Extremity Post Stroke - 0Documento22 páginasChapter 4B - Upper Extremity Post Stroke - 0Giga Hasabi AlkaraniAinda não há avaliações
- Patfis Valvular Heart DiseaseDocumento1 páginaPatfis Valvular Heart DiseaseHusna LathiifaAinda não há avaliações
- Ham D PDFDocumento1 páginaHam D PDFRabiatul AdawiyahAinda não há avaliações
- Laryngeal Motor Cortex and Control of Speech in Humans - Simonyan 2011Documento17 páginasLaryngeal Motor Cortex and Control of Speech in Humans - Simonyan 2011Maite CassanovaAinda não há avaliações
- LEAPS Fugl-Meyer InstructionsDocumento17 páginasLEAPS Fugl-Meyer InstructionsDaniele Bertolo100% (1)
- A Randomized Trial Comparing Cardiac Rehabilitation To Standard of Care For Adults With Congenital Heart DiseaseDocumento9 páginasA Randomized Trial Comparing Cardiac Rehabilitation To Standard of Care For Adults With Congenital Heart DiseaseHusna LathiifaAinda não há avaliações
- Konstipasi ICUDocumento7 páginasKonstipasi ICUHusna LathiifaAinda não há avaliações
- 1.analysis of Relationship Among The Functional ClassificationDocumento5 páginas1.analysis of Relationship Among The Functional ClassificationHusna LathiifaAinda não há avaliações
- Tmi Knee PfpsDocumento1 páginaTmi Knee PfpsHusna LathiifaAinda não há avaliações
- Spasticity Lit. Reveiw 2010Documento36 páginasSpasticity Lit. Reveiw 2010lewienAinda não há avaliações
- Comments, Opinions, and ReviewsDocumento7 páginasComments, Opinions, and ReviewsHusna LathiifaAinda não há avaliações
- Manual Therapy: Theresa Helissa Nakagawa, Carlos Dias Maciel, F Abio Viadanna Serr AoDocumento5 páginasManual Therapy: Theresa Helissa Nakagawa, Carlos Dias Maciel, F Abio Viadanna Serr AoHusna LathiifaAinda não há avaliações
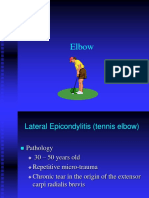
- Elbow, Wrist, HandDocumento47 páginasElbow, Wrist, HandHusna LathiifaAinda não há avaliações
- Bernhardt 20161111Documento7 páginasBernhardt 20161111Husna LathiifaAinda não há avaliações
- Wartegg Test PDFDocumento1 páginaWartegg Test PDFHusna LathiifaAinda não há avaliações
- Muscle Manual: WWW - Premierglobal.Co - UkDocumento94 páginasMuscle Manual: WWW - Premierglobal.Co - UkMilena RohenkohlAinda não há avaliações
- 6.24 Muscles Head & Neck - Blok 6Documento12 páginas6.24 Muscles Head & Neck - Blok 6magenthaAinda não há avaliações
- Body Map: Smooth or Visceral MuscleDocumento2 páginasBody Map: Smooth or Visceral MuscleFani Try Utami BoedaxRed'waterzzAinda não há avaliações
- Powerpoint Scap. Rehab Ann CoolsDocumento9 páginasPowerpoint Scap. Rehab Ann CoolsWalter PelaezAinda não há avaliações
- Muscles QuestionsDocumento3 páginasMuscles QuestionsIRADUKUNDA Marie SolangeAinda não há avaliações
- Fill in The Blanks Muscular Fitness Edition: Name: Date: PeriodDocumento2 páginasFill in The Blanks Muscular Fitness Edition: Name: Date: PeriodJack MessarosAinda não há avaliações
- The Quadratus Lumborum BlockDocumento6 páginasThe Quadratus Lumborum BlockEdwin YosuaAinda não há avaliações
- Anatomy Head and NeckDocumento25 páginasAnatomy Head and NeckMARISOL GALLEGO DUQUEAinda não há avaliações
- Kinesiology Flashcards, 3E - Lippert, Lynn S., Minor, Mary Alice Duesterhause PDFDocumento219 páginasKinesiology Flashcards, 3E - Lippert, Lynn S., Minor, Mary Alice Duesterhause PDFOrAinda não há avaliações
- Chapter 4. Muscular - System JeDocumento55 páginasChapter 4. Muscular - System JeIvonike Lim100% (2)
- Muscle Study GuideDocumento12 páginasMuscle Study GuideMitzi De Vera100% (1)
- Gastrocnemius SoleusDocumento8 páginasGastrocnemius SoleusgoldfishxAinda não há avaliações
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Documento3 páginasLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyeAinda não há avaliações
- Zogadi Cnebebi Zeda Kiduris SesaxebDocumento8 páginasZogadi Cnebebi Zeda Kiduris Sesaxebsasa sasadzeAinda não há avaliações
- The Physiologic Support SystemDocumento45 páginasThe Physiologic Support SystemModesto MasangkayAinda não há avaliações
- Anatomy of Pain Trigger Point Therapy For Exercise Professionals Exam Pack 0616Documento42 páginasAnatomy of Pain Trigger Point Therapy For Exercise Professionals Exam Pack 0616Dharmender Singh67% (3)
- BRS Gross Anatomy 7th 2012Documento506 páginasBRS Gross Anatomy 7th 20126003101008ชวิศ อาภรณ์วิรัตน์Ainda não há avaliações
- Muscular System ReviewerDocumento3 páginasMuscular System ReviewerRuffie JohnAinda não há avaliações
- Ilustrated Kinesio TapingDocumento117 páginasIlustrated Kinesio TapingNewtonBaldan94% (31)
- (Zoo301) Muscles OiaDocumento5 páginas(Zoo301) Muscles OiaRain HongAinda não há avaliações
- Special Tests in Shoulder ExaminationDocumento28 páginasSpecial Tests in Shoulder Examinationthwiseman100% (1)
- Compex Electrode PlacementDocumento2 páginasCompex Electrode PlacementIL Mago100% (2)
- What Are Similarities Between Cardiac and Skeletal MuscleDocumento3 páginasWhat Are Similarities Between Cardiac and Skeletal MuscleWafa Nabilah KamalAinda não há avaliações
- Basics of Bio Mechanics NSRDocumento30 páginasBasics of Bio Mechanics NSRAsina MilasAinda não há avaliações
- Ally Rose - Muscular SystemDocumento4 páginasAlly Rose - Muscular SystemGogo El-HawAinda não há avaliações
- PrimemoverDocumento3 páginasPrimemoverMuhammad rafif 'ulwanAinda não há avaliações
- Human Anatomy Physiology 11Th Edition Marieb Test Bank Full Chapter PDFDocumento36 páginasHuman Anatomy Physiology 11Th Edition Marieb Test Bank Full Chapter PDFninhdermotc1u100% (9)
- Plantillas Cuerpo Humano Plastilina Esqueleto OrganosDocumento13 páginasPlantillas Cuerpo Humano Plastilina Esqueleto OrganosMari Trolli JijiAinda não há avaliações
- Physioex Lab Report: Pre-Lab Quiz ResultsDocumento4 páginasPhysioex Lab Report: Pre-Lab Quiz ResultsAulia OctaviaAinda não há avaliações
- Grade - 1 Health ActivitiesDocumento82 páginasGrade - 1 Health Activitiesaimee.library.mathematicsAinda não há avaliações
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayAinda não há avaliações
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerNo EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerNota: 4 de 5 estrelas4/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindNo EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindNota: 4.5 de 5 estrelas4.5/5 (1)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouNo EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouNota: 3.5 de 5 estrelas3.5/5 (5)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingNo EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingNota: 4.5 de 5 estrelas4.5/5 (66)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionNo EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionNota: 3.5 de 5 estrelas3.5/5 (11)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicNo EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicNota: 5 de 5 estrelas5/5 (1)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!No EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Nota: 4.5 de 5 estrelas4.5/5 (22)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsNo EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsNota: 5 de 5 estrelas5/5 (96)
- Whole Body Barefoot: Transitioning Well to Minimal FootwearNo EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearNota: 4 de 5 estrelas4/5 (16)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeNo EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeNota: 4.5 de 5 estrelas4.5/5 (111)
- The Yogi Code: Seven Universal Laws of Infinite SuccessNo EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessNota: 4.5 de 5 estrelas4.5/5 (104)
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantNo EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantNota: 4.5 de 5 estrelas4.5/5 (38)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.No EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Nota: 4.5 de 5 estrelas4.5/5 (124)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesAinda não há avaliações
- Structural Integration and Energy Medicine: A Handbook of Advanced BodyworkNo EverandStructural Integration and Energy Medicine: A Handbook of Advanced BodyworkNota: 4 de 5 estrelas4/5 (1)
- The Yamas & Niyamas: Exploring Yoga's Ethical PracticeNo EverandThe Yamas & Niyamas: Exploring Yoga's Ethical PracticeNota: 4.5 de 5 estrelas4.5/5 (19)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceNo EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceNota: 4.5 de 5 estrelas4.5/5 (237)
- Fascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)No EverandFascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)Nota: 5 de 5 estrelas5/5 (3)
- The Power of Now by Eckhart Tolle: Summary and AnalysisNo EverandThe Power of Now by Eckhart Tolle: Summary and AnalysisNota: 4.5 de 5 estrelas4.5/5 (12)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingNo EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingNota: 4.5 de 5 estrelas4.5/5 (132)
- Body by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekNo EverandBody by Science: A Research Based Program to Get the Results You Want in 12 Minutes a WeekNota: 4 de 5 estrelas4/5 (38)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsNo EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsNota: 4.5 de 5 estrelas4.5/5 (7)
- Buteyko Breathing Course Manual: For use with the Advanced Buteyko CourseNo EverandButeyko Breathing Course Manual: For use with the Advanced Buteyko CourseNota: 5 de 5 estrelas5/5 (1)