Você também pode gostar
- Good Health and Well Being (Makalah Mine 2)Documento4 páginasGood Health and Well Being (Makalah Mine 2)Diva MaurizkiAinda não há avaliações
- Golongan Obat EsensialDocumento34 páginasGolongan Obat EsensialVivid Dwi Rahmadi100% (1)
- Makalah Bahasa Inggris 2Documento7 páginasMakalah Bahasa Inggris 2azizah LasimpalaAinda não há avaliações
- Bhagani 2018Documento7 páginasBhagani 2018rifky kurniawanAinda não há avaliações
- Keeping School Environment CleanDocumento3 páginasKeeping School Environment CleannashrullahadeAinda não há avaliações
- Nama PatenDocumento1 páginaNama PatenputritataAinda não há avaliações
- Laporan IPEDocumento15 páginasLaporan IPERidha FadhilaAinda não há avaliações
- Aprilia P - F3318016Documento3 páginasAprilia P - F3318016SolekAinda não há avaliações
- Adoc - Pub Harborne J B Metode Fitokimia Penuntun Cara ModernDocumento5 páginasAdoc - Pub Harborne J B Metode Fitokimia Penuntun Cara ModernFirdaAinda não há avaliações
- Taksonomi Tumbuhan 1-1Documento196 páginasTaksonomi Tumbuhan 1-1Ilham AdAinda não há avaliações
- Hubungan Tingkat Stres Perawat Dengan Kualitas Tidur Pada Pekerja Shift Malam 21.49Documento8 páginasHubungan Tingkat Stres Perawat Dengan Kualitas Tidur Pada Pekerja Shift Malam 21.49farahanisaaulia97Ainda não há avaliações
- Hubungan Tindakan Ibu Terhadap Kejadian 79bb44cbDocumento11 páginasHubungan Tindakan Ibu Terhadap Kejadian 79bb44cbAnisa SafutriAinda não há avaliações
- Contoh Soal Bahasa InggrisDocumento3 páginasContoh Soal Bahasa InggrisprasetiyoAinda não há avaliações
- CBR IlpolDocumento43 páginasCBR IlpolEykachio TariganAinda não há avaliações
- Identifikasi InfusDocumento6 páginasIdentifikasi InfusNur Zahra IkaputriAinda não há avaliações
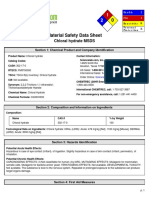
- Chloral HydrateDocumento6 páginasChloral HydrateAditya PratomoAinda não há avaliações
- Case 11. Makalah ParasitDocumento102 páginasCase 11. Makalah ParasitOki NurliantoAinda não há avaliações
- RPP Farmakognosi (Rhizoma)Documento5 páginasRPP Farmakognosi (Rhizoma)hety istiadah tsaurie100% (1)
- Hygiene Makalah Bahasa InggrisDocumento7 páginasHygiene Makalah Bahasa InggrisPutri ShabiraAinda não há avaliações
- Makalah Bahasa Inggris IIDocumento44 páginasMakalah Bahasa Inggris IIandriAinda não há avaliações
- Nama Obat Satuan Nama Obat Satuan: Daftar Obat Di Ruangan Obat Puskesmas Angsau Bulan: NO KET NO KETDocumento5 páginasNama Obat Satuan Nama Obat Satuan: Daftar Obat Di Ruangan Obat Puskesmas Angsau Bulan: NO KET NO KETMhayaNazarEvilKyuAinda não há avaliações
- Poultry As An Alternative Source of GelatinDocumento13 páginasPoultry As An Alternative Source of GelatinAlmiraRosentadewiAinda não há avaliações
- Anatomi Sistem PencernaanDocumento14 páginasAnatomi Sistem Pencernaansufita 1702Ainda não há avaliações
- Hubungan Asupan Serat Makanan Dan Cairan Dengan Kejadian Konstipasi Fungsional Pada Remaja Di Sma Kesatrian 1 SemarangDocumento10 páginasHubungan Asupan Serat Makanan Dan Cairan Dengan Kejadian Konstipasi Fungsional Pada Remaja Di Sma Kesatrian 1 SemarangHanifAinda não há avaliações
- Daftar PustakaDocumento6 páginasDaftar PustakanickyAinda não há avaliações
- Skripsi Tanpa PembahasanDocumento65 páginasSkripsi Tanpa PembahasanAddin AmrullahAinda não há avaliações
- Mini ProposalDocumento13 páginasMini ProposalSyukri Kurniawan NasutionAinda não há avaliações
- List High AlertDocumento11 páginasList High Alertputiasri85Ainda não há avaliações
- Daftar Pustaka 13Documento3 páginasDaftar Pustaka 13Angkatan 2018 FK Muhammadiyah Palembang100% (1)
- Tabitha maudy charoline medicine listDocumento9 páginasTabitha maudy charoline medicine listTabitha Maudy Charoline GintingAinda não há avaliações
- Daftar Daftar Analisa Bahan MakananDocumento12 páginasDaftar Daftar Analisa Bahan MakananFridarama DianAinda não há avaliações
- Review Jurnal Sterile CompoundingDocumento6 páginasReview Jurnal Sterile CompoundingAyu BenedictaAinda não há avaliações
- Jurnal IpcDocumento16 páginasJurnal IpcNela Yuliya DewiAinda não há avaliações
- Metabolisme Asam AminoDocumento55 páginasMetabolisme Asam AminoRommi Juliansyah0% (1)
- Jurnal Kependidikan: Implementasi Pendekatan Kontekstual Untuk Meningkatkan Gairah Siswa ..Documento13 páginasJurnal Kependidikan: Implementasi Pendekatan Kontekstual Untuk Meningkatkan Gairah Siswa ..Rinaldi Dwi CahyoAinda não há avaliações
- Semana 4 PrepositionsDocumento16 páginasSemana 4 PrepositionsEstudio Jurídico Abogadas AsociadasAinda não há avaliações
- Tugas Bahasa InggrisDocumento4 páginasTugas Bahasa InggrisBerthy BlegurAinda não há avaliações
- DAFTAR OBAT ORAL PADAT BERDASARKAN KELAS FARMAKOTERAPI DAN FAST MOVINGDocumento3 páginasDAFTAR OBAT ORAL PADAT BERDASARKAN KELAS FARMAKOTERAPI DAN FAST MOVINGlee andryAinda não há avaliações
- Review Jurnal Interaksi Obat Antihipertensi - Radhwa Fauztina (20190350050)Documento13 páginasReview Jurnal Interaksi Obat Antihipertensi - Radhwa Fauztina (20190350050)Radhwa FauztinaAinda não há avaliações
- Teori 7 Pilar Dasar IKMDocumento41 páginasTeori 7 Pilar Dasar IKMIntan Putri Wirahana ShantyAinda não há avaliações
- TyrosinaseDocumento22 páginasTyrosinaseDani Sirait0% (1)
- Rundown Acara Seminar Internasional 25Documento2 páginasRundown Acara Seminar Internasional 25Ros NilaAinda não há avaliações
- Uji Karsinogenik & MutagenikDocumento23 páginasUji Karsinogenik & MutagenikMariadi CaniagoAinda não há avaliações
- Daftar Obat Yang Dianjurkan Untuk Ibu Hamil Dan MenyusuiDocumento10 páginasDaftar Obat Yang Dianjurkan Untuk Ibu Hamil Dan Menyusuisunar4deris5413Ainda não há avaliações
- Daftar PustakaDocumento3 páginasDaftar PustakaIndrasti BanjaransariAinda não há avaliações
- Artikel Bahasa Inggris Tentang Kesehatan - Docx SeptianDocumento2 páginasArtikel Bahasa Inggris Tentang Kesehatan - Docx Septianwidy_haidaAinda não há avaliações
- Tinpus FarmakoekonomiDocumento6 páginasTinpus FarmakoekonomiYesi Widya IswariAinda não há avaliações
- Daftar Atc DDD Antibiotik Who 2018Documento12 páginasDaftar Atc DDD Antibiotik Who 2018APOTEKER RSUMMAinda não há avaliações
- Permasalahan DLM CompoundingDocumento60 páginasPermasalahan DLM CompoundingRusyda Humaira ArumaishaAinda não há avaliações
- Pengertian Quality Control Dan Quality AssuranceDocumento7 páginasPengertian Quality Control Dan Quality AssuranceNi Wayan IndrianiAinda não há avaliações
- Jurnal Sistem EndokrinDocumento9 páginasJurnal Sistem EndokrinRoby4Ainda não há avaliações
- Anesthetic Management in Emergency Exploratory Laparotomy of Perforation Peritonitis in 92 Years Old PatientDocumento3 páginasAnesthetic Management in Emergency Exploratory Laparotomy of Perforation Peritonitis in 92 Years Old PatientSarah RonquilloAinda não há avaliações
- Emergency Asthma TreatmentDocumento3 páginasEmergency Asthma TreatmentMarissita Pasillitas DopctoraAinda não há avaliações
- Case AKIDocumento5 páginasCase AKIVivi DeviyanaAinda não há avaliações
- VTE Cases For StudentsDocumento46 páginasVTE Cases For StudentsHanifah Siti AisyahAinda não há avaliações
- Pi Is 0025619611601213Documento5 páginasPi Is 0025619611601213FarmaIndasurAinda não há avaliações
- Pedoman CopdDocumento42 páginasPedoman CopddaranhtgAinda não há avaliações
- MOH DHA HAAD Dental Study Material Part 2Documento33 páginasMOH DHA HAAD Dental Study Material Part 2Junaid Ramzan89% (37)
- Volume 1, Issue 1, December 2000 - Rifampicin-Induced Acute Renal Failure and HepatitisDocumento2 páginasVolume 1, Issue 1, December 2000 - Rifampicin-Induced Acute Renal Failure and HepatitisWelki VernandoAinda não há avaliações
- Adverse Drug ReactionDocumento6 páginasAdverse Drug ReactionAranya BhandaryAinda não há avaliações
- Symptoms of MesothiliomaDocumento2 páginasSymptoms of MesothiliomaKurnilam Nur CiptaningsihAinda não há avaliações
- Mobilisasi Dan Fisioterapi-Vap PDFDocumento9 páginasMobilisasi Dan Fisioterapi-Vap PDFYANAinda não há avaliações
- Artikel Bahasa Inggris Tentang PenyakitDocumento2 páginasArtikel Bahasa Inggris Tentang PenyakitKurnilam Nur Ciptaningsih100% (1)
- Artikel Bahasa Inggris Tentang PenyakitDocumento2 páginasArtikel Bahasa Inggris Tentang PenyakitKurnilam Nur Ciptaningsih100% (1)
- Stress Dose SteroidsDocumento4 páginasStress Dose SteroidsTitien fitria sholihati100% (1)
- Clinical Evoked PotentialsDocumento13 páginasClinical Evoked PotentialsHerminaElenaAinda não há avaliações
- Tilapia 4Documento69 páginasTilapia 4Annisa MeilaniAinda não há avaliações
- Initiatives of FSSAIDocumento27 páginasInitiatives of FSSAIAshok Yadav100% (2)
- Amarin V Hikma 331 PDFDocumento284 páginasAmarin V Hikma 331 PDFMets FanAinda não há avaliações
- ICD-10 & ICD-9 codes for common medical conditions and proceduresDocumento59 páginasICD-10 & ICD-9 codes for common medical conditions and procedureskiyoeugraAinda não há avaliações
- Pedigree Analysis: (Cf. Chapters 4.4, 5.2, 6.2 of Textbook)Documento11 páginasPedigree Analysis: (Cf. Chapters 4.4, 5.2, 6.2 of Textbook)Kristyne OliciaAinda não há avaliações
- Practitioner Agreement PCP/SpecialistDocumento20 páginasPractitioner Agreement PCP/SpecialistCommunityBridgesAinda não há avaliações
- Seminar on Concepts and Foundations of RehabilitationDocumento13 páginasSeminar on Concepts and Foundations of Rehabilitationamitesh_mpthAinda não há avaliações
- Student study on family health and pregnancy in rural ZimbabweDocumento3 páginasStudent study on family health and pregnancy in rural ZimbabweTubocurareAinda não há avaliações
- EXERCISE 7 in Vitro Effects of Antimicrobial On MicroorganismsDocumento6 páginasEXERCISE 7 in Vitro Effects of Antimicrobial On MicroorganismsRachel Miranda GacutanAinda não há avaliações
- 2014 Windsor University Commencement Ceremony PROOFDocumento28 páginas2014 Windsor University Commencement Ceremony PROOFKeidren LewiAinda não há avaliações
- TH THDocumento11 páginasTH THFista Divi AmesiaAinda não há avaliações
- BurosumabDocumento8 páginasBurosumabutamiprakosoAinda não há avaliações
- Daftar Regulasi Bidang KeperawatanDocumento128 páginasDaftar Regulasi Bidang KeperawatanSanti AndrianiAinda não há avaliações
- VP ShuntDocumento5 páginasVP ShuntPradeep SharmaAinda não há avaliações
- A Novel Visual Clue For The Diagnosis of Hypertrophic Lichen PlanusDocumento1 páginaA Novel Visual Clue For The Diagnosis of Hypertrophic Lichen Planus600WPMPOAinda não há avaliações
- Tender No 38 S Haad PT 2014Documento26 páginasTender No 38 S Haad PT 2014Sundar Ramasamy100% (1)
- Practical MCQ Question For 4-YearDocumento39 páginasPractical MCQ Question For 4-Yearkhuzaima9100% (2)
- 1413272524world10 15 14 PDFDocumento38 páginas1413272524world10 15 14 PDFCoolerAdsAinda não há avaliações
- Who Trs 999 FinalDocumento292 páginasWho Trs 999 FinalfmeketeAinda não há avaliações
- Concrete MSDS 1 PDFDocumento5 páginasConcrete MSDS 1 PDFmanil_5100% (1)
- Parallax Xray For Maxillary CanineDocumento3 páginasParallax Xray For Maxillary Canineabdul samad noorAinda não há avaliações
- Rosemont Health Center Rev01Documento7 páginasRosemont Health Center Rev01Amit VishwakarmaAinda não há avaliações
- Garfinkel Case at The University of MinnesotaDocumento9 páginasGarfinkel Case at The University of MinnesotaMarkingsonCaseAinda não há avaliações
- Care for Neonatal PatientsDocumento5 páginasCare for Neonatal PatientsJonette Castro HermidaAinda não há avaliações
- Sepsis Content Concepts MapDocumento2 páginasSepsis Content Concepts Mapghodghod1230% (1)
- End users' contact and product informationDocumento3 páginasEnd users' contact and product informationمحمد ہاشمAinda não há avaliações
- 74 Manila Pest Control Vs WCCDocumento4 páginas74 Manila Pest Control Vs WCCharryAinda não há avaliações
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesNo EverandThe Ultimate Guide To Memory Improvement TechniquesNota: 5 de 5 estrelas5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementNo EverandTechniques Exercises And Tricks For Memory ImprovementNota: 4.5 de 5 estrelas4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsAinda não há avaliações
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 5 de 5 estrelas5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingNo EverandThe Happiness Trap: How to Stop Struggling and Start LivingNota: 4 de 5 estrelas4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 5 de 5 estrelas5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 3.5 de 5 estrelas3.5/5 (32)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsAinda não há avaliações
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossNo EverandThe Tennis Partner: A Doctor's Story of Friendship and LossNota: 4.5 de 5 estrelas4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNo EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNota: 5 de 5 estrelas5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)