Você também pode gostar
- Nattokinase: A Promising Alternative in Prevention and Treatment of Cardiovascular DiseasesDocumento8 páginasNattokinase: A Promising Alternative in Prevention and Treatment of Cardiovascular DiseasesVũ Đức ChiếnAinda não há avaliações
- The Grand Challenges in Cardiovascular Drug Delivery: Iwona CichaDocumento4 páginasThe Grand Challenges in Cardiovascular Drug Delivery: Iwona CichaBîkes NâçarAinda não há avaliações
- The Use of Nanotechnology in Cardiovascular DiseasDocumento13 páginasThe Use of Nanotechnology in Cardiovascular DiseasCAinda não há avaliações
- Nuevos Tratamientos IAMDocumento15 páginasNuevos Tratamientos IAMkarina hernandezAinda não há avaliações
- Pathogenesis of Atherosclerosis A Review PDFDocumento7 páginasPathogenesis of Atherosclerosis A Review PDFPrecious IJAinda não há avaliações
- Pathophysiology of Myocardial Infarction and Acute Management StrategiesDocumento11 páginasPathophysiology of Myocardial Infarction and Acute Management StrategiesnwabukingzAinda não há avaliações
- Cells 11 04136 v2Documento3 páginasCells 11 04136 v2ayunda rinataAinda não há avaliações
- Dosis DoxoDocumento12 páginasDosis DoxodeyaAinda não há avaliações
- Spath 2016Documento18 páginasSpath 2016Pratama InsaniAinda não há avaliações
- AntiagreganteDocumento19 páginasAntiagregantecAinda não há avaliações
- Stemcell CardiovascularDocumento29 páginasStemcell CardiovascularAdi WijayantoAinda não há avaliações
- Cardiovascular UltrasoundDocumento13 páginasCardiovascular UltrasoundAndi HeriAinda não há avaliações
- Dagher, Therapeutic Potential of Quercetin To Alleviate Endothelial Dysfunction in Age-Related Cardiovascular Diseases ODocumento24 páginasDagher, Therapeutic Potential of Quercetin To Alleviate Endothelial Dysfunction in Age-Related Cardiovascular Diseases ODaniel Castillo hernándezAinda não há avaliações
- The Role of Nutraceuticals in Statin Intolerant PatientsDocumento23 páginasThe Role of Nutraceuticals in Statin Intolerant PatientsJanaina Cunha Barbosa DalloAinda não há avaliações
- The Role of Oral Anticoagulant Therapy in Patients With Acute Coronary SyndromeDocumento14 páginasThe Role of Oral Anticoagulant Therapy in Patients With Acute Coronary SyndromeIntan Winta PratiwiAinda não há avaliações
- Pi Is 1053077019308778Documento2 páginasPi Is 1053077019308778Artur VianaAinda não há avaliações
- Gori, 2008Documento4 páginasGori, 2008sigiAinda não há avaliações
- A Comprehensive Review On Antithrombotic Therapy For Peripheral Artery DiseaseDocumento8 páginasA Comprehensive Review On Antithrombotic Therapy For Peripheral Artery DiseasesunhaolanAinda não há avaliações
- Jurnal 1Documento8 páginasJurnal 1Alya AlphiyantiAinda não há avaliações
- Ijms 22 10037 v2Documento30 páginasIjms 22 10037 v2deyaAinda não há avaliações
- Non-Steroidal Anti-Inflammatory Drugs For The Treatment of Pain and Immobility-Associated Osteoarthritis: Consensus Guidance For Primary CareDocumento7 páginasNon-Steroidal Anti-Inflammatory Drugs For The Treatment of Pain and Immobility-Associated Osteoarthritis: Consensus Guidance For Primary CarenabilatidaraAinda não há avaliações
- Application of Biomaterials in Cardiac Repair and RegenerationDocumento8 páginasApplication of Biomaterials in Cardiac Repair and RegenerationHadi MosaferiAinda não há avaliações
- Hyperlipidemia in Stroke Pathobiology and Therapy: Insights and PerspectivesDocumento6 páginasHyperlipidemia in Stroke Pathobiology and Therapy: Insights and Perspectivesputri aprilliaAinda não há avaliações
- Cardiology Update 2017 PDFDocumento4 páginasCardiology Update 2017 PDFFC Mekar AbadiAinda não há avaliações
- A Clinical Evaluation of Statin Pleiotropy: Statins Selectively and Dose-Dependently Reduce Vascular InflammationDocumento9 páginasA Clinical Evaluation of Statin Pleiotropy: Statins Selectively and Dose-Dependently Reduce Vascular InflammationzzakieAinda não há avaliações
- Bioinspired Yeast Microcapsules Loaded With Self-Assembled Nanotherapies For Targeted Treatment of Cardiovascular DiseaseDocumento13 páginasBioinspired Yeast Microcapsules Loaded With Self-Assembled Nanotherapies For Targeted Treatment of Cardiovascular DiseaseM.Febrian BachtiarAinda não há avaliações
- Trends in Cardiovascular Medicine: Avirup Guha, MBBS, Merna Armanious, MD, Michael G. Fradley, MDDocumento11 páginasTrends in Cardiovascular Medicine: Avirup Guha, MBBS, Merna Armanious, MD, Michael G. Fradley, MDMIGUEL MORENOAinda não há avaliações
- Nanoplumbers: Biomaterials To Fight Cardiovascular Diseases: Flavio Dormont, Mariana Varna, Patrick CouvreurDocumento22 páginasNanoplumbers: Biomaterials To Fight Cardiovascular Diseases: Flavio Dormont, Mariana Varna, Patrick CouvreurDanielAinda não há avaliações
- Cardio Onco ReviewDocumento14 páginasCardio Onco ReviewFrancisco MonzonAinda não há avaliações
- Godin2010 PDFDocumento7 páginasGodin2010 PDFLivia Maria RaduAinda não há avaliações
- 2347 6809 1 PBDocumento28 páginas2347 6809 1 PBppni lamonganAinda não há avaliações
- 2013 - STEMI - Future Strategies - LancetDocumento14 páginas2013 - STEMI - Future Strategies - LancetMichail PapafaklisAinda não há avaliações
- IbuprofenDocumento11 páginasIbuprofennephylymAinda não há avaliações
- Pathogenesis of Atherosclerosis A Review: Imedpub JournalsDocumento6 páginasPathogenesis of Atherosclerosis A Review: Imedpub JournalsHaydee RocaAinda não há avaliações
- Cannon 2006Documento11 páginasCannon 2006BENJAMIN CAMACHO SILVAAinda não há avaliações
- 1 s2.0 S0914508719301765 MainDocumento8 páginas1 s2.0 S0914508719301765 MainAdriani HartantoAinda não há avaliações
- 2017 STEMI Ehx393 - Web Addenda - For WEBDocumento8 páginas2017 STEMI Ehx393 - Web Addenda - For WEBRESCATEURAinda não há avaliações
- Nanomaterials For Drug Delivery AssignmentDocumento8 páginasNanomaterials For Drug Delivery AssignmentABDUL NAWAS K STUDENT - EEEAinda não há avaliações
- Monti 2020Documento8 páginasMonti 2020Ian MannAinda não há avaliações
- Novel-Antiplatelet Therapies For Atherothrombotic Diseases: K.malleswari, D.Rama Bramha Reddy, A.Karthikeya SharmaDocumento8 páginasNovel-Antiplatelet Therapies For Atherothrombotic Diseases: K.malleswari, D.Rama Bramha Reddy, A.Karthikeya Sharma9493.karthikAinda não há avaliações
- EMBO Mol Med - 2022 - Simats - Systemic Inflammation After Stroke Implications For Post Stroke ComorbiditiesDocumento18 páginasEMBO Mol Med - 2022 - Simats - Systemic Inflammation After Stroke Implications For Post Stroke ComorbiditiesAna GabrielaAinda não há avaliações
- Cardioprotective Effect of Coenzyme Q10 On ApoptoticDocumento6 páginasCardioprotective Effect of Coenzyme Q10 On ApoptoticJulita MelisaAinda não há avaliações
- COMPASS by RISK STRATDocumento10 páginasCOMPASS by RISK STRATMiguel GonzalezAinda não há avaliações
- Crocin Attenuates Oxidative Stress and Myocardial Infarction Injury in RatsDocumento7 páginasCrocin Attenuates Oxidative Stress and Myocardial Infarction Injury in RatsAdrian BratuAinda não há avaliações
- NIH Public Access: Author ManuscriptDocumento17 páginasNIH Public Access: Author ManuscriptCheflak KitchenAinda não há avaliações
- Ijms 22 05654Documento22 páginasIjms 22 05654Alber AvendañoAinda não há avaliações
- Unmet Needs in Chronic Pain Management The Potential Use of CurcuminDocumento6 páginasUnmet Needs in Chronic Pain Management The Potential Use of CurcuminFlorensia WodaAinda não há avaliações
- Kolkisin PathwayDocumento8 páginasKolkisin PathwayAndreas Erick HaurissaAinda não há avaliações
- Effect of Photobiomodulation in MultiplesclerosisDocumento4 páginasEffect of Photobiomodulation in MultiplesclerosisMuhammad Imam NoorAinda não há avaliações
- Hypertensionaha 117 10787Documento8 páginasHypertensionaha 117 10787Jose Enrique DelgadoAinda não há avaliações
- Prevenção de IraDocumento21 páginasPrevenção de IrajoseAinda não há avaliações
- New England Journal Medicine: The ofDocumento10 páginasNew England Journal Medicine: The ofAlina PirtacAinda não há avaliações
- WJC 6 100Documento7 páginasWJC 6 100ayub01Ainda não há avaliações
- 1 s2.0 S2772930322000175 MainDocumento7 páginas1 s2.0 S2772930322000175 MainYULISSA FLORES RONDONAinda não há avaliações
- Lee Et Al 2023 Combination Lipid Lowering Therapy in Patients Undergoing Percutaneous Coronary InterventionDocumento10 páginasLee Et Al 2023 Combination Lipid Lowering Therapy in Patients Undergoing Percutaneous Coronary InterventionKardiologi ManadoAinda não há avaliações
- Fcell 11 1148768Documento14 páginasFcell 11 1148768liobertAinda não há avaliações
- Biomedicines 09 00620Documento20 páginasBiomedicines 09 00620Pratama InsaniAinda não há avaliações
- Molecules 27 071103Documento29 páginasMolecules 27 071103sorin.morosan64Ainda não há avaliações
- DCM - Current TreatmentDocumento9 páginasDCM - Current TreatmentSri NathAinda não há avaliações
- Clinical Pathways Dan Sistem Drgs Casemix SMF Jantung & Kedokteran Vaskular Rsud Kota Cilegon 2018 Unstable Angina Pektoris (ICD 10: ..)Documento3 páginasClinical Pathways Dan Sistem Drgs Casemix SMF Jantung & Kedokteran Vaskular Rsud Kota Cilegon 2018 Unstable Angina Pektoris (ICD 10: ..)flying highAinda não há avaliações
- Goland Et Al 2016 Angiogenic Imbalance and Residual Myocardial Injury in Recovered Peripartum Cardiomyopathy PatientsDocumento7 páginasGoland Et Al 2016 Angiogenic Imbalance and Residual Myocardial Injury in Recovered Peripartum Cardiomyopathy Patientsflying highAinda não há avaliações
- Recent Advances in Pulmonary HypertensionDocumento12 páginasRecent Advances in Pulmonary Hypertensionflying highAinda não há avaliações
- Takahashi2016Documento11 páginasTakahashi2016flying highAinda não há avaliações
- 47 PH in Patient With Hyperthyroidism-Dres - Niemeyer EN PDFDocumento4 páginas47 PH in Patient With Hyperthyroidism-Dres - Niemeyer EN PDFflying highAinda não há avaliações
- Incidence of Pulmonary Hypertension in Hyperthyroid PatientsDocumento4 páginasIncidence of Pulmonary Hypertension in Hyperthyroid Patientsflying highAinda não há avaliações
- Stem CellDocumento22 páginasStem Cellflying highAinda não há avaliações
- Colloids and Surfaces B: Biointerfaces: Christina Mckee, G. Rasul ChaudhryDocumento16 páginasColloids and Surfaces B: Biointerfaces: Christina Mckee, G. Rasul Chaudhryflying highAinda não há avaliações
- Hubungan Kelas Nyha Dengan Fraksi Ejeksi Pada Pasien Gagal Jantung Kronik Di Blu/Rsup Prof. Dr. R.D. Kandou ManadoDocumento8 páginasHubungan Kelas Nyha Dengan Fraksi Ejeksi Pada Pasien Gagal Jantung Kronik Di Blu/Rsup Prof. Dr. R.D. Kandou Manadoflying highAinda não há avaliações
- Mesenchymal Stem Cells in Cardiac Regeneration: A Detailed Progress Report of The Last 6 Years (2010 - 2015)Documento25 páginasMesenchymal Stem Cells in Cardiac Regeneration: A Detailed Progress Report of The Last 6 Years (2010 - 2015)flying highAinda não há avaliações
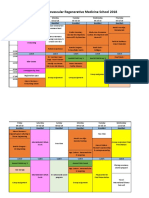
- Educational Program Cardiovascular Regenerative Medicine School 2018Documento3 páginasEducational Program Cardiovascular Regenerative Medicine School 2018flying highAinda não há avaliações
- hubungan Kadar Tnf-α Dengan Fraksi Ejeksi Pada Pasien Gagal Jantung Kronik Di Blu - rsup Prof. Dr. r.d. Kandou ManadoDocumento6 páginashubungan Kadar Tnf-α Dengan Fraksi Ejeksi Pada Pasien Gagal Jantung Kronik Di Blu - rsup Prof. Dr. r.d. Kandou Manadoflying highAinda não há avaliações
- Mesenchymal Stem Cell Paracrine Factors in Vascular Repair and RegenerationDocumento9 páginasMesenchymal Stem Cell Paracrine Factors in Vascular Repair and Regenerationflying highAinda não há avaliações
- Rupture of Vulnerable Atherosclerotic Plaques: Micrornas Conducting The Orchestra?Documento8 páginasRupture of Vulnerable Atherosclerotic Plaques: Micrornas Conducting The Orchestra?flying highAinda não há avaliações
- s2 2016 354560 BibliographyDocumento4 páginass2 2016 354560 Bibliographyflying highAinda não há avaliações
- ResearchDocumento21 páginasResearchBBD BBDAinda não há avaliações
- Metabolic SyndromeDocumento106 páginasMetabolic SyndromeLinda Hall Rothery100% (1)
- Diabetes Phils ReportDocumento89 páginasDiabetes Phils ReportRold Brio SosAinda não há avaliações
- 2501027Documento9 páginas2501027vishal makadiaAinda não há avaliações
- Jupiter Trial: DR Sheeraz Alam DM Cardiology SR1 JNMCH, AmuDocumento23 páginasJupiter Trial: DR Sheeraz Alam DM Cardiology SR1 JNMCH, AmuSheerazAinda não há avaliações
- Clerkship Handbook: Family MedicineDocumento51 páginasClerkship Handbook: Family MedicineKen WonAinda não há avaliações
- Dyslipidemia Final Poster June 24Documento2 páginasDyslipidemia Final Poster June 24drabdulrabbAinda não há avaliações
- Nejm Pcsk9 StudyDocumento10 páginasNejm Pcsk9 Studyherbertgur777Ainda não há avaliações
- Lipid Digestion and AbsorptionDocumento37 páginasLipid Digestion and AbsorptionIMDCBiochem100% (1)
- New Drug 2010 Upto Aug 2010Documento15 páginasNew Drug 2010 Upto Aug 2010NAVNEET BAGGAAinda não há avaliações
- Guidelines For The Diagnosis and Management of Heterozygous Familial Hypercholesterolemia PDFDocumento14 páginasGuidelines For The Diagnosis and Management of Heterozygous Familial Hypercholesterolemia PDFai_tAinda não há avaliações
- 2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateDocumento43 páginas2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical Updatejulioel1nico20100% (1)
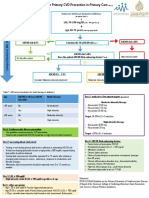
- Atherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineDocumento21 páginasAtherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineHeryanti PusparisaAinda não há avaliações
- Smart Nutrients - Abram Hoffer PDF (Orthomolecular Medicine)Documento228 páginasSmart Nutrients - Abram Hoffer PDF (Orthomolecular Medicine)Anonymous gwFqQcnaX100% (4)
- RosuvastatinDocumento17 páginasRosuvastatinddandan_2Ainda não há avaliações
- Leo Atp IvDocumento25 páginasLeo Atp IvLeonardo MedinaAinda não há avaliações
- What Really Causes High CholesterolDocumento5 páginasWhat Really Causes High CholesterolsnickoletAinda não há avaliações
- Cardiovascular Disorders: Annette HaynesDocumento69 páginasCardiovascular Disorders: Annette HaynesBinh Yen Quach TranAinda não há avaliações
- Peripheral Arterial DiseaseDocumento11 páginasPeripheral Arterial DiseaseAnas YahyaAinda não há avaliações
- Hopkins Medicine Review Cardiology SectionDocumento54 páginasHopkins Medicine Review Cardiology SectiondrsalilsidhqueAinda não há avaliações
- J Jacc 2023 02 011Documento3 páginasJ Jacc 2023 02 011Evania BeatriceAinda não há avaliações
- Ekstrak Daun Alpukat Terhadap Penurunan Kadar KolesterolDocumento5 páginasEkstrak Daun Alpukat Terhadap Penurunan Kadar Kolesterolsiti rohmaniAinda não há avaliações
- מצגת קרדיולוגיה מעודכנת עם שאלות 1Documento289 páginasמצגת קרדיולוגיה מעודכנת עם שאלות 1adnan shwAinda não há avaliações
- UntitledDocumento2 páginasUntitledJoshua Teo Beng ChinAinda não há avaliações
- Statin Therapy, Review of Safety and Potential Side EffectsDocumento9 páginasStatin Therapy, Review of Safety and Potential Side EffectsDhita Dwi NandaAinda não há avaliações
- Term 3 Rationale Pharmacology and MCNDocumento35 páginasTerm 3 Rationale Pharmacology and MCNKing KongAinda não há avaliações
- Massachusetts General Hospital (MGH) COVID-19 Treatment GuidanceDocumento24 páginasMassachusetts General Hospital (MGH) COVID-19 Treatment Guidancerajesh BAinda não há avaliações
- A Case of Severe Statin Induced IleusDocumento1 páginaA Case of Severe Statin Induced IleussnipergirlAinda não há avaliações
- 2015 The Influence of Gut Microbiota On Drug Metabolism and Toxicity. EODMTDocumento29 páginas2015 The Influence of Gut Microbiota On Drug Metabolism and Toxicity. EODMTJoseloAinda não há avaliações
- Drug ToxicityDocumento12 páginasDrug ToxicityLaeeq R MalikAinda não há avaliações
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainNo EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainNota: 4 de 5 estrelas4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNota: 4 de 5 estrelas4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (60)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (45)