Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Huntsville Businesses That Received More Than $150,000 From The Paycheck Protection ProgramDocumento14 páginasHuntsville Businesses That Received More Than $150,000 From The Paycheck Protection ProgramJonathan GrassAinda não há avaliações
- OrthosisDocumento35 páginasOrthosissinghmenkaAinda não há avaliações
- Physician Assistant Certification and Recertification Exam Review - PANRE - PANCEDocumento14 páginasPhysician Assistant Certification and Recertification Exam Review - PANRE - PANCEThe Physician Assistant Life100% (3)
- T Bringing Classical and Contemporary Homoeopathy Ogether: Research Oriented Homoeopathic ApproachDocumento107 páginasT Bringing Classical and Contemporary Homoeopathy Ogether: Research Oriented Homoeopathic ApproachVarshaAinda não há avaliações
- National policy on ambulance use and servicesDocumento6 páginasNational policy on ambulance use and servicesPatrickpeterpol Atutubo De QuirosAinda não há avaliações
- Calcaneum Fractures: Jensen Joseph GMC KannurDocumento104 páginasCalcaneum Fractures: Jensen Joseph GMC KannurAmel VnairAinda não há avaliações
- Pest Control Risk Assessment Indoor and OutdoorDocumento72 páginasPest Control Risk Assessment Indoor and OutdoorarmkarthickAinda não há avaliações
- Monoclonal Antibodies and Engineered AntibodiesDocumento24 páginasMonoclonal Antibodies and Engineered AntibodiesMunawar AliAinda não há avaliações
- Cooler (E-216)Documento26 páginasCooler (E-216)Suci Nur RachmiAinda não há avaliações
- HBVGuidance Terrault Et Al-2018-Hepatology PDFDocumento40 páginasHBVGuidance Terrault Et Al-2018-Hepatology PDFAnonymous wdmpgxAinda não há avaliações
- Electroconvulsive Therapy in Functional Hallucination Scope and ChallengesDocumento3 páginasElectroconvulsive Therapy in Functional Hallucination Scope and ChallengesSuci Nur RachmiAinda não há avaliações
- Decision Making and Support Available To Individuals Considering and Undertaking Electroconvulsive Therapy (ECT)Documento9 páginasDecision Making and Support Available To Individuals Considering and Undertaking Electroconvulsive Therapy (ECT)Suci Nur RachmiAinda não há avaliações
- Resume Jurnal-Dessy Dwi H 201720401011160Documento3 páginasResume Jurnal-Dessy Dwi H 201720401011160Pratiwi UmbohAinda não há avaliações
- Arriving at The Scene: Initial Response/Prioritization of Efforts 2.safety ProceduresDocumento2 páginasArriving at The Scene: Initial Response/Prioritization of Efforts 2.safety ProceduresSumit GuptaAinda não há avaliações
- Kinesiology Elbow Joint PDFDocumento8 páginasKinesiology Elbow Joint PDFRozyAinda não há avaliações
- Depression in Today - BioDocumento5 páginasDepression in Today - Bioapi-272648963Ainda não há avaliações
- Science Blood TransfusionsDocumento10 páginasScience Blood Transfusionsapi-237866019Ainda não há avaliações
- Medicine in Situ Panchen TraditionDocumento28 páginasMedicine in Situ Panchen TraditionJigdrel77Ainda não há avaliações
- HSPK 2021Documento270 páginasHSPK 2021Sabrina Agustien SimanungkalitAinda não há avaliações
- FISIOGRAFT ENG Set 17 PDFDocumento28 páginasFISIOGRAFT ENG Set 17 PDFmaxAinda não há avaliações
- Abigail BDocumento3 páginasAbigail BbjhilarioAinda não há avaliações
- FORMAT Discharge PlanDocumento5 páginasFORMAT Discharge PlanButchay LumbabAinda não há avaliações
- Pulmonary EmbolismDocumento93 páginasPulmonary EmbolismRakesh PanchalAinda não há avaliações
- Hesi v2Documento125 páginasHesi v2kandiezein88Ainda não há avaliações
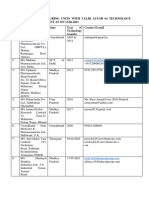
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Documento5 páginasList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesAinda não há avaliações
- Unit-V Chapter 20. Breathing and Exchange of Gases: Important PointsDocumento13 páginasUnit-V Chapter 20. Breathing and Exchange of Gases: Important PointsminaAinda não há avaliações
- Scio Four Gas Module Family: Reliable and Flexible Gas AnalysisDocumento2 páginasScio Four Gas Module Family: Reliable and Flexible Gas AnalysisNasr Eldin AlyAinda não há avaliações
- Konsep Latihan Plyometric PDFDocumento27 páginasKonsep Latihan Plyometric PDFDwinda Abi PermanaAinda não há avaliações
- What Type of Resistance Training Program Can Help Increase Muscle MassDocumento75 páginasWhat Type of Resistance Training Program Can Help Increase Muscle Massyokimura dimaunahanAinda não há avaliações
- Pasteurized EggsDocumento8 páginasPasteurized Eggsapi-202950260Ainda não há avaliações
- Navidas-Case StudyDocumento5 páginasNavidas-Case StudyFran LanAinda não há avaliações
- Medical Certificate Guidelines June 2012Documento3 páginasMedical Certificate Guidelines June 2012wudthipanAinda não há avaliações
- Joint InfectionsDocumento10 páginasJoint InfectionsJPAinda não há avaliações