Você também pode gostar
- Infectious Disease - Antibiotic Ladder PDFDocumento2 páginasInfectious Disease - Antibiotic Ladder PDFVaishali PrasharAinda não há avaliações
- Pance Prep Pearls AntibioticsDocumento14 páginasPance Prep Pearls Antibioticskat100% (4)
- Adult Infectious Disease Bulletpoints HandbookNo EverandAdult Infectious Disease Bulletpoints HandbookNota: 4.5 de 5 estrelas4.5/5 (9)
- Adhesive Capsulitis Presentation May 2009Documento29 páginasAdhesive Capsulitis Presentation May 2009cm4100% (1)
- Antiobitic Infection TX ChartDocumento8 páginasAntiobitic Infection TX ChartTLAinda não há avaliações
- 90+% of S. Aureus Are Resistant To PCN: Clinical PearlsDocumento6 páginas90+% of S. Aureus Are Resistant To PCN: Clinical PearlsJessica WoeppelAinda não há avaliações
- Antibiotics - Who Kills WhatDocumento1 páginaAntibiotics - Who Kills WhatBenHansonAinda não há avaliações
- Print Antibiotics ReviewDocumento6 páginasPrint Antibiotics ReviewtiuwangAinda não há avaliações
- Antibiotic Class by CoverageDocumento3 páginasAntibiotic Class by Coverageayy1Ainda não há avaliações
- Antibiotic Management Chalk Talk NotesDocumento3 páginasAntibiotic Management Chalk Talk NotesMarl KarxAinda não há avaliações
- Pharmacology II 352 CDocumento15 páginasPharmacology II 352 CMustafa SaßerAinda não há avaliações
- Veterinary Antimicrobial DrugsDocumento5 páginasVeterinary Antimicrobial DrugsLaureece Salm ApduhanAinda não há avaliações
- O DOC For Syphillis (Benzathine Penicillin), o DOC in Strep Infections, Especially To Prevent Rheumatic Fever o DOC For Susceptible PneumococciDocumento5 páginasO DOC For Syphillis (Benzathine Penicillin), o DOC in Strep Infections, Especially To Prevent Rheumatic Fever o DOC For Susceptible PneumococciIndu BhavanaAinda não há avaliações
- Penicillins - KatzungDocumento6 páginasPenicillins - KatzungKarl CAinda não há avaliações
- Antibioticsforyear3medics PDFDocumento13 páginasAntibioticsforyear3medics PDFShonaMalhanAinda não há avaliações
- Antibacterial DR Mostafa Alfishawy AntibioticDocumento64 páginasAntibacterial DR Mostafa Alfishawy Antibioticramzi MohamedAinda não há avaliações
- Introduction To AntibioticsDocumento6 páginasIntroduction To AntibioticsMuslimAinda não há avaliações
- HCC Exam 4Documento20 páginasHCC Exam 4Sheri BarlingAinda não há avaliações
- The Beta-Lactam Antibiotics: Cell Wall Active AgentsDocumento32 páginasThe Beta-Lactam Antibiotics: Cell Wall Active Agentsjayaprakashr72616Ainda não há avaliações
- Opportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaDocumento4 páginasOpportunistic Mycoses: Portal of Entry: Respiratory, Mucocutaneous Infectious Particles: Conidia, MyceliaPinay YaunAinda não há avaliações
- Antibiotic TableDocumento1 páginaAntibiotic Tablebob someoneAinda não há avaliações
- Case 1: Toxacara CatiDocumento4 páginasCase 1: Toxacara Catiseo82087Ainda não há avaliações
- Antimicrobial PANCE ReviewDocumento40 páginasAntimicrobial PANCE ReviewFlora LawrenceAinda não há avaliações
- Topic - Neutropenic Fever OutlineDocumento5 páginasTopic - Neutropenic Fever Outlineapi-549451092Ainda não há avaliações
- Sketchy Pharm - AntimicrobialsDocumento32 páginasSketchy Pharm - AntimicrobialsDennis Torres SchelamaussAinda não há avaliações
- 1a Antiinfective DrugsDocumento4 páginas1a Antiinfective DrugsMaria Donabella OngueAinda não há avaliações
- Cephalosporins Quick ReviewDocumento19 páginasCephalosporins Quick ReviewErinson Custodio PlasenciaAinda não há avaliações
- Tropical Medicine Lecture Edited-1Documento96 páginasTropical Medicine Lecture Edited-1inspiredwriter617Ainda não há avaliações
- Antibiotic Summary - DraftDocumento10 páginasAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Supporting Document of How To Choose Empirical Antibiotics in ICU Video LectureDocumento7 páginasSupporting Document of How To Choose Empirical Antibiotics in ICU Video LectureNeha AgrawalAinda não há avaliações
- Clinical Pharmacology - Rationale Behind Antibiotics PrescriptionDocumento12 páginasClinical Pharmacology - Rationale Behind Antibiotics PrescriptionhalesAinda não há avaliações
- Antibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsDocumento12 páginasAntibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsMuath AlqarniAinda não há avaliações
- InfectionDocumento96 páginasInfectionBassem Georguos LabibAinda não há avaliações
- BDS and NUR Two Antiprotozoal MarchDocumento68 páginasBDS and NUR Two Antiprotozoal MarchElvis KiprotichAinda não há avaliações
- Microbiology Summary DocumentDocumento7 páginasMicrobiology Summary DocumentKAinda não há avaliações
- Pharm: Antibacteria/Antiviral/AntifungalDocumento19 páginasPharm: Antibacteria/Antiviral/AntifungalNathan BarrerasAinda não há avaliações
- 2011 PK-PD AntibiotikDocumento88 páginas2011 PK-PD AntibiotikUniatimelindaAinda não há avaliações
- Antibacterials For Respiratory Tract Infections: Cecilia C. Maramba-Lazarte, MD, MscidDocumento29 páginasAntibacterials For Respiratory Tract Infections: Cecilia C. Maramba-Lazarte, MD, MscidCecile Maramba-LazarteAinda não há avaliações
- Infectious Diseases of The Dog and CatDocumento52 páginasInfectious Diseases of The Dog and CatHikmat UllahAinda não há avaliações
- Bacteriology SummaryDocumento35 páginasBacteriology SummarykevinAinda não há avaliações
- Antibiotics: Penicillium-Terrestrial Mold Cephalosporium - Marine Mold Bacillus - Bacteria Streptomyces - BacteriaDocumento9 páginasAntibiotics: Penicillium-Terrestrial Mold Cephalosporium - Marine Mold Bacillus - Bacteria Streptomyces - BacteriavexicaAinda não há avaliações
- Classification of Clinically Significant Bacteria by GenusDocumento2 páginasClassification of Clinically Significant Bacteria by GenusSEAN BUIAinda não há avaliações
- Classification of Clinically Significant Bacteria by GenusDocumento2 páginasClassification of Clinically Significant Bacteria by GenusBrhmcmicroAinda não há avaliações
- Bacteria: Gram + CoverDocumento2 páginasBacteria: Gram + CoverPhil St Flour NPMT Central CoastAinda não há avaliações
- 4 IGP Basics of Antimicrobial TherapyDocumento11 páginas4 IGP Basics of Antimicrobial TherapyTin NatividadAinda não há avaliações
- DR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Documento33 páginasDR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Astria PermanaAinda não há avaliações
- Common Antibiotic UseDocumento40 páginasCommon Antibiotic UseKittiphat ChaikuntaAinda não há avaliações
- Rangkuman UkaiDocumento15 páginasRangkuman Ukaimaxifarma2023Ainda não há avaliações
- USMLE Step 3 Lecture Notes 2017-2018Documento74 páginasUSMLE Step 3 Lecture Notes 2017-2018kaelenAinda não há avaliações
- 7fa8e6ac-47db-4f0f-90f3-bb6e1ece863cDocumento18 páginas7fa8e6ac-47db-4f0f-90f3-bb6e1ece863cSatendra SrivastavaAinda não há avaliações
- Rapid Review AntibioticsDocumento82 páginasRapid Review AntibioticsObaroAinda não há avaliações
- Group I: Penicillin G (Benzylpenicillin), Penicillin V (Phenoxymethylpenicillin)Documento16 páginasGroup I: Penicillin G (Benzylpenicillin), Penicillin V (Phenoxymethylpenicillin)jhk451Ainda não há avaliações
- AntibacterialsDocumento8 páginasAntibacterialslisalynnleeAinda não há avaliações
- Parasites and Parasitism (Parasitology)Documento3 páginasParasites and Parasitism (Parasitology)Joraine Nichole Roquero VillajuanAinda não há avaliações
- Antimicrobials IDocumento40 páginasAntimicrobials IclarkfunAinda não há avaliações
- Antibiotics: Faculty of Dentistry 22 September 2014Documento61 páginasAntibiotics: Faculty of Dentistry 22 September 2014gamalsolimanAinda não há avaliações
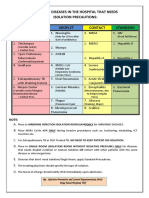
- Diseases That Needs Isolation PrecautionsDocumento1 páginaDiseases That Needs Isolation Precautionsjerimiah_manzonAinda não há avaliações
- DermatologyDocumento29 páginasDermatologykeyur patelAinda não há avaliações
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Documento38 páginas2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALAinda não há avaliações
- Wound CX: NGTD Day 1, Upon D/C Long Term Abx IV Vs PO - Given History of Recurrently UTI, Will Get CT Abd/pelvis To R/o Underlying PathologyDocumento2 páginasWound CX: NGTD Day 1, Upon D/C Long Term Abx IV Vs PO - Given History of Recurrently UTI, Will Get CT Abd/pelvis To R/o Underlying PathologyBenHansonAinda não há avaliações
- Usmle Step 1 240, Step 2 244 Comlex Level 1 604, Level 2 618 Class Rank Top Quartile Ecs/Research Were WeakDocumento5 páginasUsmle Step 1 240, Step 2 244 Comlex Level 1 604, Level 2 618 Class Rank Top Quartile Ecs/Research Were WeakBenHansonAinda não há avaliações
- Visiting Student Application Service (VSAS)Documento10 páginasVisiting Student Application Service (VSAS)BenHansonAinda não há avaliações
- Cardiology - ACLS Easy PDFDocumento1 páginaCardiology - ACLS Easy PDFrolpf garriAinda não há avaliações
- USMLE Step 1 Study Plan 2Documento3 páginasUSMLE Step 1 Study Plan 2BenHansonAinda não há avaliações
- MATUCOL 3 Meses Seguridad Efectividad de Metodos de InduccionDocumento11 páginasMATUCOL 3 Meses Seguridad Efectividad de Metodos de InduccionMitsury Jacqueline Flores C.Ainda não há avaliações
- Burns SeminarDocumento66 páginasBurns SeminarPratibha Thakur100% (1)
- Lesson 4Documento6 páginasLesson 4doldol ocampoAinda não há avaliações
- Drug StudyDocumento3 páginasDrug StudySherlyn Delos ReyesAinda não há avaliações
- Urinary Tract Infection (UTI) : Pharmacotherapeutics II YrDocumento20 páginasUrinary Tract Infection (UTI) : Pharmacotherapeutics II YrpawannnnAinda não há avaliações
- Muscular System FunctionDocumento2 páginasMuscular System FunctionLachlan PalmerAinda não há avaliações
- Chapter 46 Antianginal AgentsDocumento14 páginasChapter 46 Antianginal AgentsJewel SantosAinda não há avaliações
- Grade 6: The Heart and Circulatory SystemDocumento18 páginasGrade 6: The Heart and Circulatory SystemEstanislao Villanueva ElemAinda não há avaliações
- Open Heart Surgery CaabgDocumento6 páginasOpen Heart Surgery CaabgGopi KrishnanAinda não há avaliações
- Desvenlafaxine Venlafaxine: StructureDocumento6 páginasDesvenlafaxine Venlafaxine: StructureAndrew PanickerAinda não há avaliações
- HPV Template MasterlistDocumento1 páginaHPV Template Masterlistmarialovella.gonzagaAinda não há avaliações
- 10.master Rotation Plan M. Sc. Nursing 1st YearDocumento4 páginas10.master Rotation Plan M. Sc. Nursing 1st YearNaresh JeengarAinda não há avaliações
- Gastrointestinal System Practice ExamDocumento53 páginasGastrointestinal System Practice Examcarina.pldtAinda não há avaliações
- J1-T5 Anemia FerropénicaDocumento12 páginasJ1-T5 Anemia FerropénicaGoblin HunterAinda não há avaliações
- Physiotherapy Management of TMJ PainDocumento4 páginasPhysiotherapy Management of TMJ Painakheel ahammed100% (1)
- Metastases Bone DiseaseDocumento59 páginasMetastases Bone Diseasemuhammad rustamAinda não há avaliações
- 9c5ff54e-92aa-4393-8350-218e91c128d2Documento6 páginas9c5ff54e-92aa-4393-8350-218e91c128d2Zarbakht AliAinda não há avaliações
- Tarife AnalizeDocumento1 páginaTarife AnalizeVincze Alina ClaudiaAinda não há avaliações
- Ischemic Optic NeuropathyDocumento10 páginasIschemic Optic NeuropathyScerbatiuc CristinaAinda não há avaliações
- User Guide For The Participant Use Data File: American College of Surgeons National Surgical Quality Improvement ProgramDocumento40 páginasUser Guide For The Participant Use Data File: American College of Surgeons National Surgical Quality Improvement Programbobobobo12341212Ainda não há avaliações
- ADAT Practice TestDocumento54 páginasADAT Practice TestRyan GrossAinda não há avaliações
- Case PresentationDocumento10 páginasCase Presentationapi-402129690Ainda não há avaliações
- Rachel Costa ResumeDocumento2 páginasRachel Costa ResumeracrnAinda não há avaliações
- Cir 0000000000000549Documento120 páginasCir 0000000000000549MSAinda não há avaliações
- Medstar ObGyn 2nd EditionDocumento570 páginasMedstar ObGyn 2nd EditionMerahit Abera100% (2)
- Respiratory MCQs LJDocumento7 páginasRespiratory MCQs LJfjghAinda não há avaliações
- Kanker PayudaraDocumento2 páginasKanker PayudaraIndrawati SyarifAinda não há avaliações
- AAST Renal Injury ScaleDocumento11 páginasAAST Renal Injury ScaleyuenkeithAinda não há avaliações
- GGT enDocumento2 páginasGGT enKaoueche OmarAinda não há avaliações