Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Solution Leads To Better Learning, Even When Errors: ChaptersDocumento5 páginasSolution Leads To Better Learning, Even When Errors: ChaptersGisselle PauloAinda não há avaliações
- Chapters: by Robert T. KiyosakiDocumento4 páginasChapters: by Robert T. KiyosakiGisselle PauloAinda não há avaliações
- CDSCSCDSCDVFDocumento2 páginasCDSCSCDSCDVFGisselle PauloAinda não há avaliações
- 6 SurgeryDocumento4 páginas6 SurgeryGisselle PauloAinda não há avaliações
- Food Expenses: Not IncludedDocumento3 páginasFood Expenses: Not IncludedGisselle PauloAinda não há avaliações
- Homes Schools Workplaces City Centers Neighborhoods ParksDocumento3 páginasHomes Schools Workplaces City Centers Neighborhoods ParksGisselle PauloAinda não há avaliações
- Solution Leads To Better Learning, Even When Errors: ChaptersDocumento5 páginasSolution Leads To Better Learning, Even When Errors: ChaptersGisselle PauloAinda não há avaliações
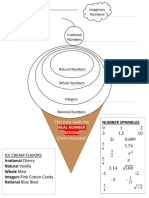
- Thinking of Ice Cream: Imaginary Numbers The Number SystemDocumento1 páginaThinking of Ice Cream: Imaginary Numbers The Number SystemGisselle Paulo0% (1)
- Chapters: The Dream of The PlanetDocumento17 páginasChapters: The Dream of The PlanetGisselle PauloAinda não há avaliações
- (PEDIA) HN6 Toddler & Middle 2Documento4 páginas(PEDIA) HN6 Toddler & Middle 2Gisselle PauloAinda não há avaliações
- INDIVIDUAL, Written - Time Allotment: Elimination RoundsDocumento1 páginaINDIVIDUAL, Written - Time Allotment: Elimination RoundsGisselle PauloAinda não há avaliações
- 50cm 1.7 20g/day Doubled BW Tripled BW BL +50% Increase Delayed Eruption 1.3 1Documento5 páginas50cm 1.7 20g/day Doubled BW Tripled BW BL +50% Increase Delayed Eruption 1.3 1Gisselle PauloAinda não há avaliações
- 05 Pedia & Adolescent CareDocumento3 páginas05 Pedia & Adolescent CareGisselle PauloAinda não há avaliações
- Color Coded Grade LevelsDocumento2 páginasColor Coded Grade LevelsGisselle PauloAinda não há avaliações
- Form No. 212 Revised Personal Data Sheet - NewDocumento14 páginasForm No. 212 Revised Personal Data Sheet - NewGisselle PauloAinda não há avaliações
- SkincareDocumento1 páginaSkincareGisselle PauloAinda não há avaliações
- Laundry List: Received byDocumento2 páginasLaundry List: Received byGisselle PauloAinda não há avaliações
- INDIVIDUAL, Written - Time Allotment: Elimination RoundsDocumento1 páginaINDIVIDUAL, Written - Time Allotment: Elimination RoundsGisselle PauloAinda não há avaliações
- Must Know FindingsDocumento4 páginasMust Know FindingsGisselle PauloAinda não há avaliações
- Preschool Preschool Preschool Preschool: Preschool Preschool Preschool PreschoolDocumento1 páginaPreschool Preschool Preschool Preschool: Preschool Preschool Preschool PreschoolGisselle PauloAinda não há avaliações
- Worksheet - Number System PDFDocumento1 páginaWorksheet - Number System PDFGisselle PauloAinda não há avaliações
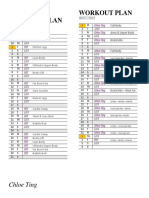
- 42 Day ChallengeDocumento1 página42 Day ChallengeGisselle PauloAinda não há avaliações
- University of Santo Tomas Faculty of Medicine & Surgery: Section 1CDocumento2 páginasUniversity of Santo Tomas Faculty of Medicine & Surgery: Section 1CGisselle PauloAinda não há avaliações
- Alg 1-GHS Syllabus 2015-2016Documento4 páginasAlg 1-GHS Syllabus 2015-2016Gisselle PauloAinda não há avaliações
- Foshay Learning Center: 6 Grade Math Class SyllabusDocumento2 páginasFoshay Learning Center: 6 Grade Math Class SyllabusGisselle PauloAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Industrial Hygiene Guidance PDFDocumento84 páginasIndustrial Hygiene Guidance PDFNora0% (1)
- Nursing Selection TestDocumento3 páginasNursing Selection TestHarshita GuptaAinda não há avaliações
- NCP OsteosarcomaDocumento6 páginasNCP OsteosarcomaNiksAinda não há avaliações
- 2009 Fee ScheduleDocumento1.123 páginas2009 Fee ScheduleNicole HillAinda não há avaliações
- 2015 Book Dyslipidemias PDFDocumento525 páginas2015 Book Dyslipidemias PDFvaleriaovando100% (1)
- The Ayurvedic Pharmacopoeia of India: Part - Ii (Formulations) Volume - I First Edition Monographs Ebook V.1.0Documento187 páginasThe Ayurvedic Pharmacopoeia of India: Part - Ii (Formulations) Volume - I First Edition Monographs Ebook V.1.0VinitSharmaAinda não há avaliações
- Persuasive Speech Outline - Marijauna FinalDocumento4 páginasPersuasive Speech Outline - Marijauna Finalapi-34805003388% (17)
- IV. Recognizing National Issues and Concern - E-Substance Abuse EducationDocumento9 páginasIV. Recognizing National Issues and Concern - E-Substance Abuse EducationMicsjadeCastillo0% (1)
- M010-MSI-HSE-00-PLN-02007 - Rev5 Heat Stress & Summer Working Plan PDFDocumento66 páginasM010-MSI-HSE-00-PLN-02007 - Rev5 Heat Stress & Summer Working Plan PDFEldhose VargheseAinda não há avaliações
- 1) Correction of Single Gene Defect Diseases Recessive Inborn Errors ofDocumento6 páginas1) Correction of Single Gene Defect Diseases Recessive Inborn Errors ofesam889Ainda não há avaliações
- Bowel PreparationDocumento20 páginasBowel Preparationrosybash100% (1)
- Code of Practice On: Workplace Safety and Health (WSH) Risk ManagementDocumento51 páginasCode of Practice On: Workplace Safety and Health (WSH) Risk Managementaminul islamAinda não há avaliações
- Rheumatology: With Kartik Rangaraj MDDocumento39 páginasRheumatology: With Kartik Rangaraj MDNailahRahmahAinda não há avaliações
- Lesson Plan On Pituitary Gland (Endocrine SystemDocumento37 páginasLesson Plan On Pituitary Gland (Endocrine SystemRosalyn Angcay Quintinita100% (1)
- Key Points: Information About Your Procedure From The British Association of Urological Surgeons (BAUS)Documento6 páginasKey Points: Information About Your Procedure From The British Association of Urological Surgeons (BAUS)diva aurelliaAinda não há avaliações
- RLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionDocumento57 páginasRLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionAlexa GoteraAinda não há avaliações
- G2-Acute-Pancreatitis (Revised)Documento45 páginasG2-Acute-Pancreatitis (Revised)patriciaAinda não há avaliações
- Tenses Modals E-YDS 2019: Yds Kampi - İsmail TurasanDocumento7 páginasTenses Modals E-YDS 2019: Yds Kampi - İsmail TurasanAlihan GökAinda não há avaliações
- Hand Tool ReportDocumento6 páginasHand Tool ReportD.k. Asad100% (1)
- Effect of Full Crown Preparation On Pulpal Blood Flow in Man. Marisa Sukapattee. 2016. Archives of Oral BiologyDocumento6 páginasEffect of Full Crown Preparation On Pulpal Blood Flow in Man. Marisa Sukapattee. 2016. Archives of Oral BiologyValeria CrespoAinda não há avaliações
- Chapter 3 Animal Tissues SolutionDocumento6 páginasChapter 3 Animal Tissues SolutionLucky ErrojuAinda não há avaliações
- Eastfeeding StuartMacadamDocumento80 páginasEastfeeding StuartMacadamDiana Fernanda Espinosa SerranoAinda não há avaliações
- OPfr4 2Documento13 páginasOPfr4 26E Rivera Cervantes Osiris MargaritaAinda não há avaliações
- Neuromuscular BlockersDocumento25 páginasNeuromuscular BlockersAbdelrahman GalalAinda não há avaliações
- Fibroadenoma Mammae of The BreastDocumento15 páginasFibroadenoma Mammae of The Breastirvanie100% (1)
- Evolution of Aortic Arches in VertebratesDocumento2 páginasEvolution of Aortic Arches in Vertebratesarbazkhan825lAinda não há avaliações
- Comprehensive Review of Chest Tube Management A ReviewDocumento6 páginasComprehensive Review of Chest Tube Management A ReviewCesar LinaresAinda não há avaliações
- P.E EssayDocumento2 páginasP.E EssayMia LucinaAinda não há avaliações
- NCP For PTSDDocumento3 páginasNCP For PTSDjhaze09100% (4)
- 2015-07-14 RASD Workshop-Discussion Paper ODE OCD FinalDocumento30 páginas2015-07-14 RASD Workshop-Discussion Paper ODE OCD FinalShayne JacobsonAinda não há avaliações