Você também pode gostar
- Complimentary JournalDocumento58 páginasComplimentary JournalMcKey ZoeAinda não há avaliações
- Automotive E-Coat Paint Process Simulation Using FEADocumento20 páginasAutomotive E-Coat Paint Process Simulation Using FEAflowh_100% (1)
- Science and Health WritingDocumento28 páginasScience and Health WritingMark Christian CatapangAinda não há avaliações
- Canterburytales-No Fear PrologueDocumento10 páginasCanterburytales-No Fear Prologueapi-261452312Ainda não há avaliações
- Experimenting The Bactericidal Capability of Coleus Blumei (Mayana) Leaves Against S. Aureus, K. Pneumoniae and P. AeruginosaDocumento26 páginasExperimenting The Bactericidal Capability of Coleus Blumei (Mayana) Leaves Against S. Aureus, K. Pneumoniae and P. AeruginosaCarlo F. AgasAinda não há avaliações
- Medicinal Plants in Asia and Pacific for Parasitic Infections: Botany, Ethnopharmacology, Molecular Basis, and Future ProspectNo EverandMedicinal Plants in Asia and Pacific for Parasitic Infections: Botany, Ethnopharmacology, Molecular Basis, and Future ProspectAinda não há avaliações
- The Produce Contamination Problem: Causes and SolutionsNo EverandThe Produce Contamination Problem: Causes and SolutionsNota: 5 de 5 estrelas5/5 (1)
- Genetically Engineered Food: Changing the Nature of Nature: What You Need to Know to Protect Yourself, Your Family, and Our PlanetNo EverandGenetically Engineered Food: Changing the Nature of Nature: What You Need to Know to Protect Yourself, Your Family, and Our PlanetAinda não há avaliações
- So You Want To Be A NeurosugeonDocumento10 páginasSo You Want To Be A NeurosugeonColby TimmAinda não há avaliações
- Professional Builder - Agosto 2014Documento32 páginasProfessional Builder - Agosto 2014ValAinda não há avaliações
- Oreilly Design For Voice InterfacesDocumento37 páginasOreilly Design For Voice InterfacesHarmony JordenAinda não há avaliações
- Intelligent Transportation System SolutionsDocumento38 páginasIntelligent Transportation System SolutionsWisnu AjiAinda não há avaliações
- The Pros and Cons of BiotechnologyDocumento10 páginasThe Pros and Cons of Biotechnologymorethan5minutesAinda não há avaliações
- Final EditedDocumento31 páginasFinal Editedlaehaaaa40% (5)
- Surface Coating ProcessesDocumento7 páginasSurface Coating ProcessesSailabala ChoudhuryAinda não há avaliações
- Symbolic InteractionismDocumento8 páginasSymbolic InteractionismNice tuazonAinda não há avaliações
- Bacteria Research Paper TopicsDocumento5 páginasBacteria Research Paper Topicsgbjtjrwgf100% (1)
- Julie Bui - What Is Biotechnology Biomedical Science WebquestDocumento7 páginasJulie Bui - What Is Biotechnology Biomedical Science Webquestapi-522650514Ainda não há avaliações
- Flawed Scientific Studies Block Progress and Sow Confusion: GM Crops & FoodDocumento6 páginasFlawed Scientific Studies Block Progress and Sow Confusion: GM Crops & FoodperunicaAinda não há avaliações
- Thesis Antibiotic ResistanceDocumento7 páginasThesis Antibiotic ResistanceTracy Hill100% (2)
- Reading HW 3 - Summary Completion, Flow Chart Completion and Note CompletionDocumento19 páginasReading HW 3 - Summary Completion, Flow Chart Completion and Note CompletionLachayagari Harsha vardhanAinda não há avaliações
- How Not To Evaluate Augmentative Biological ControlDocumento4 páginasHow Not To Evaluate Augmentative Biological ControlVictor Lauro Perez GarciaAinda não há avaliações
- Information About CancersDocumento8 páginasInformation About CancersBogdan NeguleasaAinda não há avaliações
- Answer The Following Questions Briefly: 25 Points: NOPUETO, Keana Marcelle C. Fodma5Documento2 páginasAnswer The Following Questions Briefly: 25 Points: NOPUETO, Keana Marcelle C. Fodma5KEANA MARCELLE NOPUETOAinda não há avaliações
- Peptic Ulcer Research Paper PDFDocumento8 páginasPeptic Ulcer Research Paper PDFscxofyplg100% (1)
- Research Paper On Molecular BiologyDocumento5 páginasResearch Paper On Molecular Biologymoykicvnd100% (1)
- The Status of Biological Control and Recommendations For Improving Uptake For The FutureDocumento13 páginasThe Status of Biological Control and Recommendations For Improving Uptake For The FutureMaría Mónica Bonilla PáezAinda não há avaliações
- Ebola Research Paper ThesisDocumento7 páginasEbola Research Paper Thesisdianawalkermilwaukee100% (2)
- Antiangiogenic ThesisDocumento35 páginasAntiangiogenic ThesisCharlie M LozaritaAinda não há avaliações
- Biobanking in The PhilippinesDocumento17 páginasBiobanking in The PhilippinesLeidi Chua BayudanAinda não há avaliações
- MEDICINE MODULE 2013 BIOETHICS AND GENETICS LABS 4-6Documento6 páginasMEDICINE MODULE 2013 BIOETHICS AND GENETICS LABS 4-6Daniel MaysAinda não há avaliações
- Research Paper On YeastDocumento6 páginasResearch Paper On Yeasthnpawevkg100% (1)
- Bioethics Author(s) : Lawrence Koehler Source: Bios, Vol. 68, No. 3 (Sep., 1997), Pp. 137-141 Published By: Stable URL: Accessed: 17/06/2014 11:06Documento6 páginasBioethics Author(s) : Lawrence Koehler Source: Bios, Vol. 68, No. 3 (Sep., 1997), Pp. 137-141 Published By: Stable URL: Accessed: 17/06/2014 11:06Carlos MeneguiniAinda não há avaliações
- Q&A Plant PhysiologyDocumento202 páginasQ&A Plant PhysiologyLhu CerdonAinda não há avaliações
- How To Do Biology CourseworkDocumento8 páginasHow To Do Biology Courseworkbotav1nakak3100% (2)
- Workshop 2020Documento12 páginasWorkshop 2020AJMRAinda não há avaliações
- Mushroom Cultivation ManualDocumento101 páginasMushroom Cultivation ManualAkinwumiAinda não há avaliações
- STS Module 9Documento14 páginasSTS Module 9Claire Jacynth FloroAinda não há avaliações
- Research Paper Outline On GmosDocumento9 páginasResearch Paper Outline On Gmosafeaatrhk100% (1)
- Book Project CapstoneDocumento4 páginasBook Project Capstoneapi-606096817Ainda não há avaliações
- Gut Biome Research Opens New Frontier in MedicineDocumento7 páginasGut Biome Research Opens New Frontier in Medicinechatkat66Ainda não há avaliações
- Science, Technology & Society)Documento4 páginasScience, Technology & Society)Mcjan GuecoAinda não há avaliações
- Bioethics FixDocumento4 páginasBioethics FixMuchamad Bagus SAinda não há avaliações
- Stem Cells, Glyconutrients and The ControversyDocumento3 páginasStem Cells, Glyconutrients and The Controversysweethealth100% (1)
- Mindset For IELTS Level 3 Student - S Book-Pages-37-39Documento3 páginasMindset For IELTS Level 3 Student - S Book-Pages-37-39Phuong CaoAinda não há avaliações
- Human Genetic Enhancements Research PaperDocumento12 páginasHuman Genetic Enhancements Research Paperapi-235903650Ainda não há avaliações
- An Infectiouse Cure Help GuideDocumento11 páginasAn Infectiouse Cure Help Guidemicrofreek100% (13)
- Genetic Engineering Term PaperDocumento4 páginasGenetic Engineering Term Paperafdtywgdu100% (1)
- Term Paper Due 6 5Documento15 páginasTerm Paper Due 6 5api-340739010Ainda não há avaliações
- Batasan Hills National High School: K. Pneumoniae and P. AeruginosaDocumento28 páginasBatasan Hills National High School: K. Pneumoniae and P. AeruginosaCarlo F. AgasAinda não há avaliações
- FinalsynthesispaperDocumento16 páginasFinalsynthesispaperapi-360838252Ainda não há avaliações
- Candida Albicans Is A Fungus That Is Part of The Normal Microbiota of MostDocumento3 páginasCandida Albicans Is A Fungus That Is Part of The Normal Microbiota of MostMadiAinda não há avaliações
- Biotechnology (Week 1) 1c0Documento29 páginasBiotechnology (Week 1) 1c0Sharon CordovaAinda não há avaliações
- PETA BIOLOGY 2Documento2 páginasPETA BIOLOGY 2Sharmaine BalnegAinda não há avaliações
- The Good, The Bad, and The Dangers of Unregulated Genetic EngineeringDocumento9 páginasThe Good, The Bad, and The Dangers of Unregulated Genetic Engineeringapi-338364297Ainda não há avaliações
- VBQ-XII - Biology - Unit VIII-Biology in Human WelfareDocumento4 páginasVBQ-XII - Biology - Unit VIII-Biology in Human Welfarepradeep mathurAinda não há avaliações
- Elliott Chan B4 ELCT RE 2023 - Google DocsDocumento7 páginasElliott Chan B4 ELCT RE 2023 - Google Docs2tsAinda não há avaliações
- Philippine Medicinal Plants in Common Use - Their Phytochemistry & PharmacologyDocumento100 páginasPhilippine Medicinal Plants in Common Use - Their Phytochemistry & Pharmacologyvallery quaint100% (1)
- Chapter 1Documento7 páginasChapter 1Edwin DatanAinda não há avaliações
- The Advantages and Disadvantages of BiotechnologyDocumento3 páginasThe Advantages and Disadvantages of BiotechnologyAnushka VijayvargiyaAinda não há avaliações
- Research Paper Topics Agricultural ExtensionDocumento7 páginasResearch Paper Topics Agricultural Extensionfvj892xr100% (1)
- Research Papers On Plant Tissue CultureDocumento6 páginasResearch Papers On Plant Tissue Cultureeh041zef100% (1)
- Bioethics Social SciencesDocumento110 páginasBioethics Social Sciencesalexeiev14790Ainda não há avaliações
- Emerging Technologies For Integrated Pest Management: Crop Protection April 2001Documento3 páginasEmerging Technologies For Integrated Pest Management: Crop Protection April 20017238 Nguyễn Tường VyAinda não há avaliações
- Candida Albicans Is A Fungus That Is Part of The Normal Microbiota of MostDocumento3 páginasCandida Albicans Is A Fungus That Is Part of The Normal Microbiota of MostMadiAinda não há avaliações
- Activity #1 STSDocumento8 páginasActivity #1 STSMicah BratzAinda não há avaliações
- Thesis Statement On GM FoodsDocumento4 páginasThesis Statement On GM Foodsaflpaftaofqtoa100% (2)
- Capstone LRDocumento7 páginasCapstone LRBrian LuyahanAinda não há avaliações
- Vascular Basic Shapes in TaxonomyDocumento109 páginasVascular Basic Shapes in TaxonomykuldeepdeepikaAinda não há avaliações
- Nativo 75 WGDocumento6 páginasNativo 75 WGkuldeepdeepikaAinda não há avaliações
- GCS - 1505 - HR Web PDFDocumento16 páginasGCS - 1505 - HR Web PDFkuldeepdeepikaAinda não há avaliações
- 2015 Calendar Landscape in ColorDocumento1 página2015 Calendar Landscape in ColorkuldeepdeepikaAinda não há avaliações
- Societies 03 00147Documento11 páginasSocieties 03 00147kuldeepdeepikaAinda não há avaliações
- ICAR's Shoddy ScienceDocumento4 páginasICAR's Shoddy SciencekuldeepdeepikaAinda não há avaliações
- Climate Change and Plant DiseasesDocumento1 páginaClimate Change and Plant DiseaseskuldeepdeepikaAinda não há avaliações
- AAO Paper 2Documento16 páginasAAO Paper 2kuldeepdeepikaAinda não há avaliações
- Assistant Agriculture Officer-2011 Paper-IiDocumento1 páginaAssistant Agriculture Officer-2011 Paper-IikuldeepdeepikaAinda não há avaliações
- Agricultural R&DDocumento6 páginasAgricultural R&Dkuldeepdeepika100% (1)
- Dealing With Crop Stresses and ScandalsDocumento4 páginasDealing With Crop Stresses and ScandalskuldeepdeepikaAinda não há avaliações
- NCPP 2013-DGRDocumento2 páginasNCPP 2013-DGRkuldeepdeepikaAinda não há avaliações
- Linkage Between Science and Public Policy Has Weakened PDFDocumento2 páginasLinkage Between Science and Public Policy Has Weakened PDFkuldeepdeepikaAinda não há avaliações
- Dealing With Crop Stresses and ScandalsDocumento4 páginasDealing With Crop Stresses and ScandalskuldeepdeepikaAinda não há avaliações
- Researching Agriculture June 2013Documento54 páginasResearching Agriculture June 2013kuldeepdeepikaAinda não há avaliações
- Mupf 2012Documento45 páginasMupf 2012kuldeepdeepikaAinda não há avaliações
- Ten Simple Rules CollectionDocumento56 páginasTen Simple Rules CollectionkuldeepdeepikaAinda não há avaliações
- Abunance Biofertilizer CyanobactDocumento4 páginasAbunance Biofertilizer CyanobactkuldeepdeepikaAinda não há avaliações
- FOCARS ReadingMaterialDocumento578 páginasFOCARS ReadingMaterialkuldeepdeepikaAinda não há avaliações
- A New Disease of Bell Pepper (Capsicum Annuum Var. Grossum) Caused by Drechslera Bicolor, Its Pathophysiology, Efficacy of Fungicides and BotanicalsDocumento5 páginasA New Disease of Bell Pepper (Capsicum Annuum Var. Grossum) Caused by Drechslera Bicolor, Its Pathophysiology, Efficacy of Fungicides and BotanicalskuldeepdeepikaAinda não há avaliações
- Nagarjuna Agrichem Products RangeDocumento3 páginasNagarjuna Agrichem Products Rangekuldeepdeepika100% (1)
- Elisa TestDocumento9 páginasElisa Testbrkica2011Ainda não há avaliações
- ICAR Hindi SabdkoshDocumento37 páginasICAR Hindi Sabdkoshguru9anandAinda não há avaliações
- ARS Rules Regulations ICAR NAARMDocumento165 páginasARS Rules Regulations ICAR NAARMSridhar Gutam80% (5)
- Climate Change Will Affect Plant Pests and Diseases in The Same Way It Affects Infectious Disease AgentsDocumento19 páginasClimate Change Will Affect Plant Pests and Diseases in The Same Way It Affects Infectious Disease AgentskuldeepdeepikaAinda não há avaliações
- 3rd Global CircularDocumento9 páginas3rd Global CircularkuldeepdeepikaAinda não há avaliações
- Frac List of Fungicide Common Names - 2010Documento5 páginasFrac List of Fungicide Common Names - 2010kuldeepdeepikaAinda não há avaliações
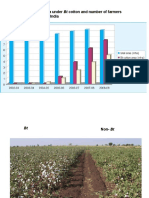
- Total Cotton Area, Area Under BT Cotton and Number of Farmers Adopting BT Cotton in IndiaDocumento5 páginasTotal Cotton Area, Area Under BT Cotton and Number of Farmers Adopting BT Cotton in IndiakuldeepdeepikaAinda não há avaliações
- Email EtiquetteDocumento4 páginasEmail EtiquettekuldeepdeepikaAinda não há avaliações
- Effect of Dust On The Performance of Wind Turbines PDFDocumento12 páginasEffect of Dust On The Performance of Wind Turbines PDFJallal ArramachAinda não há avaliações
- Canopen-Lift Shaft Installation: W+W W+WDocumento20 páginasCanopen-Lift Shaft Installation: W+W W+WFERNSAinda não há avaliações
- Sexual & Reproductive Health of AdolocentsDocumento8 páginasSexual & Reproductive Health of AdolocentsSourav HossenAinda não há avaliações
- 4D - Yulianti Viviana - Exercise 9Documento7 páginas4D - Yulianti Viviana - Exercise 9Uli JennerAinda não há avaliações
- Reading in Philippine History (Chapter 3)Documento14 páginasReading in Philippine History (Chapter 3)AKIO HIROKIAinda não há avaliações
- Direction: Read The Questions Carefully. Write The Letters of The Correct AnswerDocumento3 páginasDirection: Read The Questions Carefully. Write The Letters of The Correct AnswerRomyross JavierAinda não há avaliações
- FED - Summer Term 2021Documento18 páginasFED - Summer Term 2021nani chowdaryAinda não há avaliações
- Math-149 MatricesDocumento26 páginasMath-149 MatricesKurl Vincent GamboaAinda não há avaliações
- Chapter 4. Quality Service and Standards TrainingDocumento40 páginasChapter 4. Quality Service and Standards TrainingJia Mae Sapico ApantiAinda não há avaliações
- The Case of Ataraxia and Apraxia in The Development of Skeptic THDocumento11 páginasThe Case of Ataraxia and Apraxia in The Development of Skeptic THeweAinda não há avaliações
- Financial Services : An OverviewDocumento15 páginasFinancial Services : An OverviewAnirudh JainAinda não há avaliações
- Activity 2Documento5 páginasActivity 2Kier VillegasAinda não há avaliações
- 4 Exploring Your Personality Q and Scoring Key (Transaction Analysis)Documento3 páginas4 Exploring Your Personality Q and Scoring Key (Transaction Analysis)Tarannum Yogesh DobriyalAinda não há avaliações
- Kara&Suoglu ProjectreportDocumento4 páginasKara&Suoglu ProjectreportRicard Comas xacnóAinda não há avaliações
- Technology & Livelihood Education: WEEK 6-7Documento28 páginasTechnology & Livelihood Education: WEEK 6-7my musicAinda não há avaliações
- NewTrendsInLeadershipandManagement ArikkokDocumento32 páginasNewTrendsInLeadershipandManagement Arikkoksocofem288Ainda não há avaliações
- Cat TSDDocumento55 páginasCat TSDvarsha sharmaAinda não há avaliações
- Ir Pc-1: Pre-Check (PC) Design Criteria For Freestanding Signs and Scoreboards: 2019 CBCDocumento15 páginasIr Pc-1: Pre-Check (PC) Design Criteria For Freestanding Signs and Scoreboards: 2019 CBCAbrar AhmadAinda não há avaliações
- FeatureSelectionAccepted IEEE Review PDFDocumento20 páginasFeatureSelectionAccepted IEEE Review PDFrvsamy80Ainda não há avaliações
- Ifatsea Atsep Brochure 2019 PDFDocumento4 páginasIfatsea Atsep Brochure 2019 PDFCondor GuatonAinda não há avaliações
- MacEwan APA 7th Edition Quick Guide - 1Documento4 páginasMacEwan APA 7th Edition Quick Guide - 1Lynn PennyAinda não há avaliações