Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
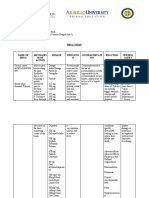
- MetronidazoleDocumento2 páginasMetronidazoleMartha Glorie Manalo WallisAinda não há avaliações
- Musculoskeletal System - Ii: MBBS Year-3 (Academic Year 2020-2021)Documento26 páginasMusculoskeletal System - Ii: MBBS Year-3 (Academic Year 2020-2021)Danyal AzamAinda não há avaliações
- Fatty LiverDocumento2 páginasFatty LivernagadeepkAinda não há avaliações
- Book GoodPracticeInPediatricAndAdolDocumento256 páginasBook GoodPracticeInPediatricAndAdolAndrea Lopez100% (2)
- Denas Book Engl 2006 PDFDocumento138 páginasDenas Book Engl 2006 PDFParallaxsterAinda não há avaliações
- ICD 10 Volume 3 - Alfabet PDFDocumento779 páginasICD 10 Volume 3 - Alfabet PDFDediAinda não há avaliações
- Review: Emilio Perucca, Piero Perucca, H Steve White, Elaine C WirrellDocumento12 páginasReview: Emilio Perucca, Piero Perucca, H Steve White, Elaine C WirrellFernandoAinda não há avaliações
- Blood and Tissue NematodesDocumento60 páginasBlood and Tissue NematodesDanielle Pecson100% (1)
- Tylenol - Acetaminophen - Fabros, JennyDocumento3 páginasTylenol - Acetaminophen - Fabros, JennyJenny Agustin FabrosAinda não há avaliações
- CNUR823 - Module 4 PDFDocumento20 páginasCNUR823 - Module 4 PDFAumAinda não há avaliações
- Journal of Clinical and Translational Endocrinology: Case ReportsDocumento5 páginasJournal of Clinical and Translational Endocrinology: Case ReportsKartikaa YantiiAinda não há avaliações
- Acute Exacerbations of Pulmonary DiseasesDocumento258 páginasAcute Exacerbations of Pulmonary DiseasesOxana TurcuAinda não há avaliações
- Edema: Pendrik Tandean Internal Medicine, Medical Faculty of Hasanuddin University, MakassarDocumento31 páginasEdema: Pendrik Tandean Internal Medicine, Medical Faculty of Hasanuddin University, MakassarLIEBERKHUNAinda não há avaliações
- @pharmaidea: Table of Metric WeightDocumento21 páginas@pharmaidea: Table of Metric WeightLaila KhanAinda não há avaliações
- Gastrointestinal Diseases: Clinical Pharmacist Hasan BayashotDocumento117 páginasGastrointestinal Diseases: Clinical Pharmacist Hasan BayashotRawabi SalehAinda não há avaliações
- Maternal Child Nursing Care in Canada 2Nd Edition Perry Test Bank Full Chapter PDFDocumento36 páginasMaternal Child Nursing Care in Canada 2Nd Edition Perry Test Bank Full Chapter PDFChristopherHugheswpya100% (12)
- Neuro Board Exam StrategiesDocumento8 páginasNeuro Board Exam StrategiesshanuddinAinda não há avaliações
- Antidepressants, Antihistamines, General Anesthetics, MAO Inhibitors, OpioidsDocumento3 páginasAntidepressants, Antihistamines, General Anesthetics, MAO Inhibitors, Opioidskaycelyn jimenezAinda não há avaliações
- Autoimmune Hemolytic AnemiaDocumento4 páginasAutoimmune Hemolytic AnemiaSamuel WibowoAinda não há avaliações
- Deep Vein ThrombosisDocumento19 páginasDeep Vein ThrombosisDoctor MusicAinda não há avaliações
- Manipura ChakraDocumento4 páginasManipura ChakraGopikrishnan RadhakrishnanAinda não há avaliações
- Mechanisms of Hypoxemia: Review ArticleDocumento14 páginasMechanisms of Hypoxemia: Review ArticleJhon CruzAinda não há avaliações
- The Gynecologic History and Pelvic Examination Up To Date 2016Documento14 páginasThe Gynecologic History and Pelvic Examination Up To Date 2016Mateo GlAinda não há avaliações
- An Update On The Novel and Approved Drugs For Alzheimer DiseaseDocumento10 páginasAn Update On The Novel and Approved Drugs For Alzheimer DiseasePAULA ITZEL AVALOS POLANCOAinda não há avaliações
- A Magnetic Resonance Imaging DEFINITIONDocumento22 páginasA Magnetic Resonance Imaging DEFINITIONYosie Yulanda PutraAinda não há avaliações
- Feb Recalls 3Documento3 páginasFeb Recalls 3reethu mammenAinda não há avaliações
- Respiratory AcidosisDocumento5 páginasRespiratory Acidosisapi-376421583% (6)
- Ophtho BookDocumento181 páginasOphtho BookSymss MathewAinda não há avaliações
- Psoas - Ultrasound CasesDocumento4 páginasPsoas - Ultrasound CasesMAYAinda não há avaliações
- Pato Sakit Kritis PDFDocumento44 páginasPato Sakit Kritis PDFrsia fatimahAinda não há avaliações